
Abstract
Background:
Although COVID-19 has contributed to more than 5 million deaths worldwide, the quality of life (QOL) for survivors should be addressed and managed. COVID-19 survivors that develop ARDS have been reported to experience impaired 6-min walk distance (6MWD) and severe fatigue, decreasing QOL. There are suggestions that exercise training significantly improves exercise capacity in COVID-19 patients, with pulmonary function testing (PFT) improving after 6 weeks of pulmonary rehabilitation (PR), contesting this QOL decline. PR has improved the QOL in other respiratory diseased patient populations. Our objective is to determine if PR benefits functional ability and quality of life for post-COVID-19 patients by increasing 6MWD and decreasing shortness of breath scores (UCSD). We hypothesize that completing 6 weeks of PR will decrease UCSD and increase 6MWD for patients with continuing dyspnea post-COVID-19 infection.
Methods:
We performed a retrospective analysis of EMR (electronic medical record) data of 47 patients diagnosed with COVID-19 who completed 6 weeks of PR at UTMB’s (University of Texas Medical Branch at Galveston) Post-COVID-19 Clinic. We compared UCSD scores and 6MWD, as measured of QOL, before and after 6 weeks of PR. Inclusion criteria were patients with positively diagnosis for COVID-19, 18 years of age or older, who completed 6 weeks of PR at UTMB’s Post-COVID-19 Clinic. Measures included PR as independent variable, UCSD, and 6MWD as outcome variables and covariates (age, gender, BMI, race/ethnicity, and PFT status). Linear regression analysis was performed to estimate the effect of PR on the UCSD score and 6MWD difference (before and after PR) controlling for all covariates.
Results:
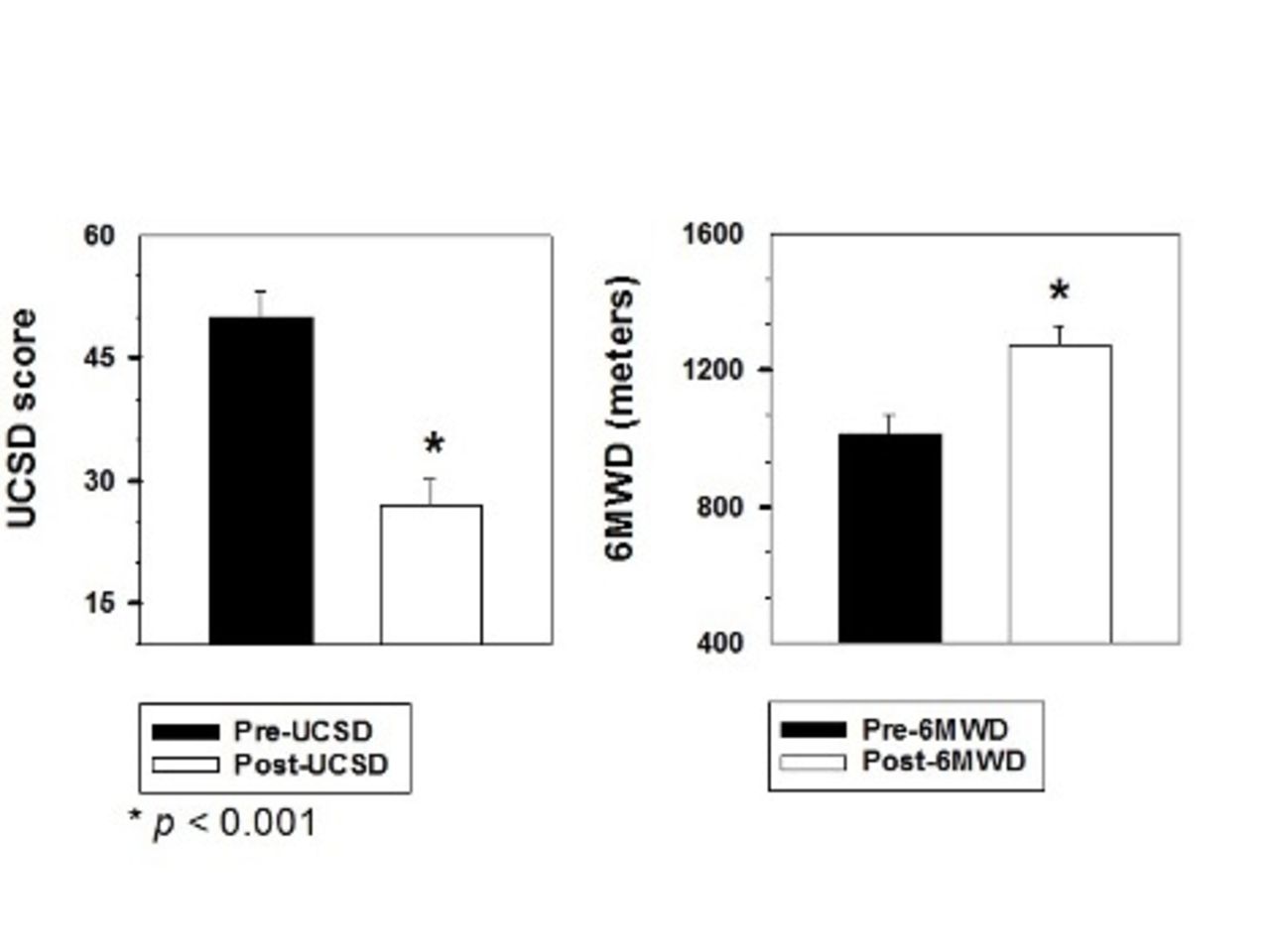
Among the patients included, 8 (59.6%) females and 19 (40.4%) males with an average of 56 ± 13 years old. There was a clinically significant improvement in QOL based on improved mean difference in UCSD -22 ± 19; and increased 6MWD mean difference 264 ± 237 m after PR. The linear regression analysis did not show any statistically significant variables associated with 6MWD. Non-Hispanic Blacks had 20.7 times higher UCSD score difference compared to non-Hispanic whites when controlling for all other variables.
Conclusions:
Measures impacting QOL and physical function, UCSD, and 6MWD, clinically improved after 6 weeks of PR for patients with continuing dyspnea post-COVID-19 infection.
BMI - Body Mass Index; UCSD - shortness of breath score; 6MWD - 6 minute walk distance in meters; Pre - before pulmonary rehabilitation; Post - after pulmonary rehabilitation
View all access options for this article.Table 1: Descriptive Statistics
Category
All Patients (n=47)
Normal Lung Function (n=24)
Obstructive/Restrictive (n= 23)
Age mean ± SD
56 ± 13
54 ± 13
58 ± 13
Gender n (%)
Male
19 (40.4)
7 (29.2)
12 (52.2)
Female
28 (59.6)
17 (70.8)
11 (47.8)
Ethnicity n (%)
Non-Hispanic White
26 (55.3)
13 (54.2)
13 (56.5)
Non-Hispanic Black
10 (21.3)
3 (12.5)
7 (30.4)
Hispanic
11 (23.4)
8 (33.3)
3 (13.0)
BMI mean ± SD
35 ± 9
34 ± 9
36 ± 10
UCSD Pre mean ± SD
50 ± 22
50 ± 23
49 ± 22
UCSD Post mean ± SD
27 ± 21
27 ± 19
27 ± 24
UCSD Difference mean ± SD
-22 ± 19
-22 ± 16
-22 ± 22
6MWD Pre (meters) mean ± SD
1011 ± 380
1063 ± 303
956 ± 447
6MWD Post (meters) mean ± SD
1275 ± 382
1346 ± 289
1200 ± 453
6MWD Difference (meters) mean ± SD
264 ± 237
283 ± 262
245 ± 213
Get full access to this article