
Abstract
Background:
Profound hypoxemia noted by an PaO2/FIO2 ratio <100 torr has been a common occurrence in COVID-19 ARDS. To address this severe hypoxemia common interventions included prone positioning, optimizing PEEP, administration of a neuromuscular paralytic, and the inhalation of nitric oxide at 20 ppm or a nebulized prostacyclin. The role of inhaled nitric oxide in ARDS is often utilized a bridge therapy until oxygenation is optimized or until another clinical interventions, example ECMO, are implemented. Rebound hypoxemia is a rare occurrence in the adult patient population occurring 2% of time. Sudden discontinuation of inhaled NO can cause severe rebound pulmonary hypertension, an increase in intrapulmonary right-to-left shunting, and a decreased PaO2. It has been suggested that downregulation of endogenous NO synthesis and/or elevated endothelin-1 levels by inhaled NO is responsible in part for this rebound phenomenon.
Methods:
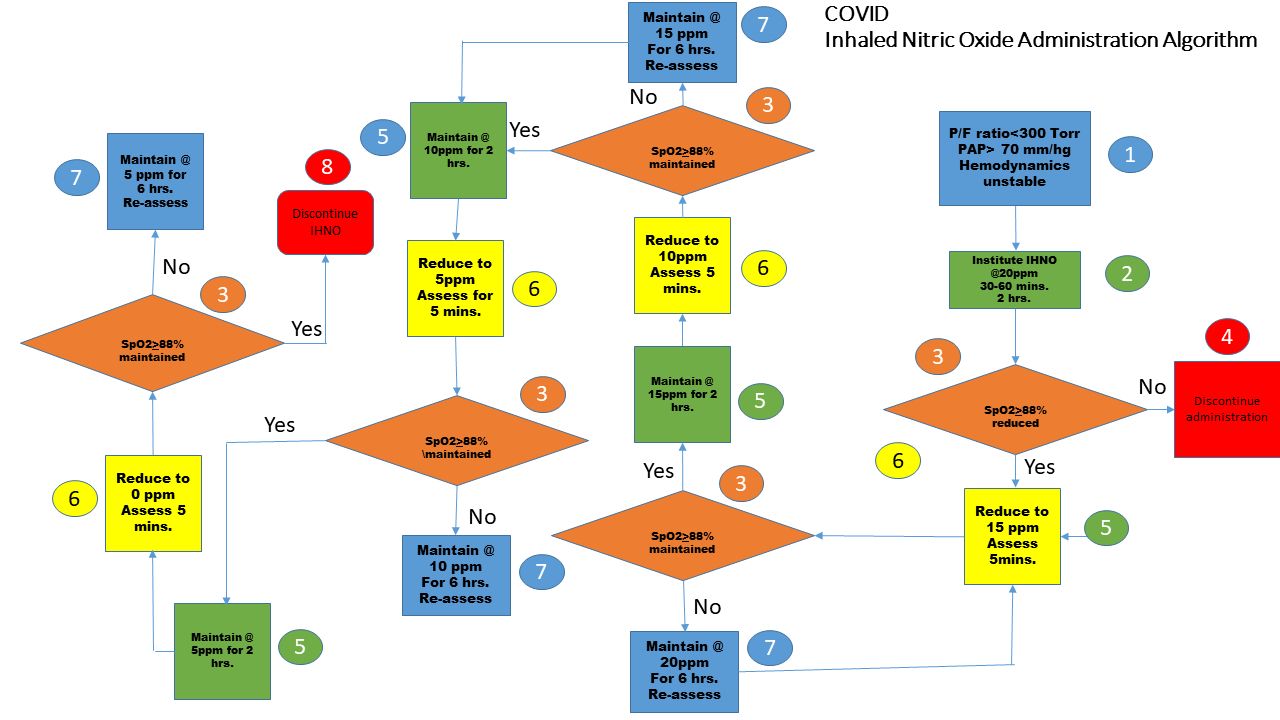
At our institution this was often the role of inhaled nitric oxide administration, however in several patients its administration was continued beyond two weeks. Weaning of inhaled nitric oxide was performed via the institution’s established titration protocol. (Fig 1)
Results:
Ten (n = 20) developed profound desaturation, (reduction in baseline SpO2 by 10%) when it was reduced below 5 ppm, requiring either an increase back to 10 ppm per protocol or increased of ventilator oxygen delivery by 20-30%. All patients were eventually weaned from nitric oxide within a 48-hour time frame. However, 4 patients required nitric oxide administration for an addition 7 days until discontinuation.
Conclusions:
The mechanism of desaturation in the COVID-19 patient population is still being postulated, the precise underlying mechanisms remain to be elucidated, to avoid rebound pulmonary hypertension, a slow, stepwise reduction of the inhaled NO concentration is recommended based our intuition’s experiences. Clinicians should be aware of quick desaturations in prolonged nitric oxide administration of the COVID-19 patient population and the interventions needed to improve the patient’s oxygenation status quickly.
Get full access to this article
View all access options for this article.