
Abstract
Background:
Our pediatric hospital utilizes 12 respiratory therapists (RTs) to perform spirometry studies in outpatient environments. The National Board of Respiratory Care (NBRC) offers the Pulmonary Function Technologist (PFT) credential for RTs to highlight specialized skills and excellence for those who obtain it. In our facility, 5 RTs were PFT certified (C/RPFT) prior to 2020 and 7 RTs became PFT certified in 2020 (2 CPFT and 5 RPFT). The quality of spirometry is guided by the American Thoracic Society (ATS) standards to ensure that spirometry results are accurately interpreted and influence care appropriately. Audits pre and post PFT credential were reviewed for acceptability based on ATS standards (Table 1). We aimed to evaluate if PFT credential achievement would translate into increased ATS compliance for spirometries performed in our pediatric hospital.
Methods:
In an IRB approved retrospective analysis, we reviewed and compared spirometry audits from 01/2019–05/2021 for compliance to ATS Standards. As part of our standard quality assurance process a minimum 30% of spirometries are randomly selected and audited by trained PFT staff for compliance based. We evaluated compliance results pre and post PFT credential achievement for the 7 RTs who obtained certification in 2020 and analyzed for differences.
Results:
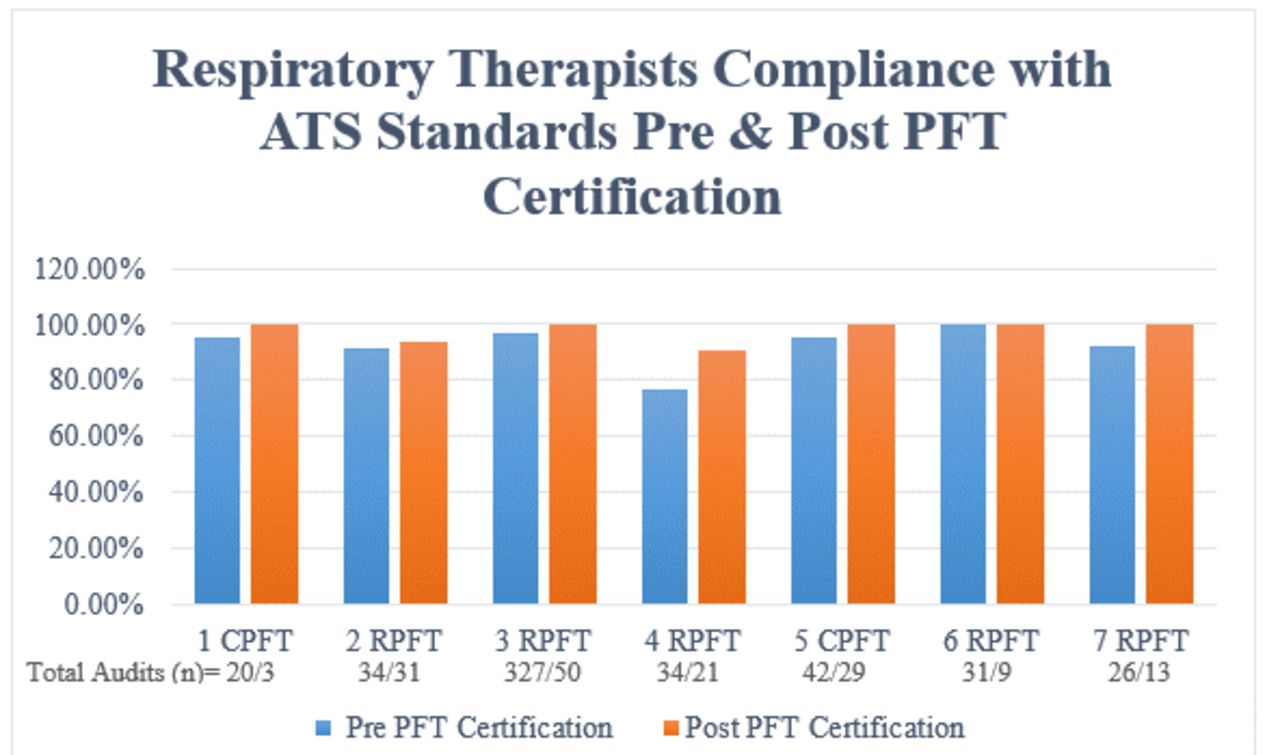
670 spirometry audits were included for analysis for the seven RTs who achieved a PFT credential in 2020 (514 pre credential and 156 post credential). Prior to PFT credential obtainment, RTs performed spirometry that met ATS standards 92.45% of the time. After obtaining PFT credential RTs performed spirometry that met ATS standards 97.72% of the time (Figure 1). This resulted in a 5.27% (P >0.05) increase in compliance with ATS standards post PFT credential achievement.
Conclusions:
In our pediatric health system, we found that spirometry compliance to ATS standards increased after RTs obtained their PFT credential. This translates into increased spirometry accuracy and could influence appropriate treatment. More research is needed to assess further implications from possible increased spirometry accuracy and the subsequent care provided.
Table 1 displays the criteria that must be met during spirometry audits in order for the spirometry to be considered in compliance with ATS standards.
Figure 1 shows the individual percentage of compliance with ATS standards for pediatric spirometry in our facility based on pre & post PFT credential achievement. View all access options for this article.Auditing Criteria for Acceptable Spirometry Based on ATS Standards
2005 ATS Criteria for an Acceptable Test
Satisfactory start of test:
1. Extrapolated volume < 5% of the FVC or 0.150 whichever is greater 2. For children 6 and younger extrapolated volume 12.5 % of FVC or 0.080L
Satisfactory end of test:
Performs the test with a maximum inhalation, good start, and smooth continuous exhalation with maximum effort:1. No cough in the first second2. No Valsalva maneuver3. No hesitation during the test4. No leaks5. No obstructed mouthpiece6. Plateau in the volume time curve
Acceptable & Repeatable:
1. Minimum of 3 similar loops2. Difference between the largest and the next largest FVC & FEV1 ≤ .150L 3. Patients with FVC <1.0L the difference between the largest and the next largest FVC & FEV1 ≤ 0.100L
Get full access to this article