
Abstract
Background:
Spirometry is a physiological test that measures how a patient inhales or exhales gas as a function of time. The American Thoracic Society (ATS) guides spirometry standards to ensure that spirometry results are accurately interpreted and influence care appropriately. Accuracy of pediatric spirometry ranges from 37-95%.1,2 In our health system, Registered Nurses (RNs) and Registered Respiratory Therapists perform pediatric spirometry. Audits of completed spirometry are reviewed by trained PFT staff for acceptability based on ATS Standards (Table 1). We reviewed audit results to evaluate for differences based on provider credential type.
Methods:
In an IRB approved retrospective analysis, we reviewed and compared pediatric spirometry audits from 11/2019-03/2020. Audits were split into groups based on credentials of the spirometry technician (RPFT, RRT, CPFT, RN). We analyzed the spirometry audits for alignment with ATS standards based on spirometry technician user. 60 RN preformed spirometries and 60 RT preformed spirometries were randomly selected and compared.
Results:
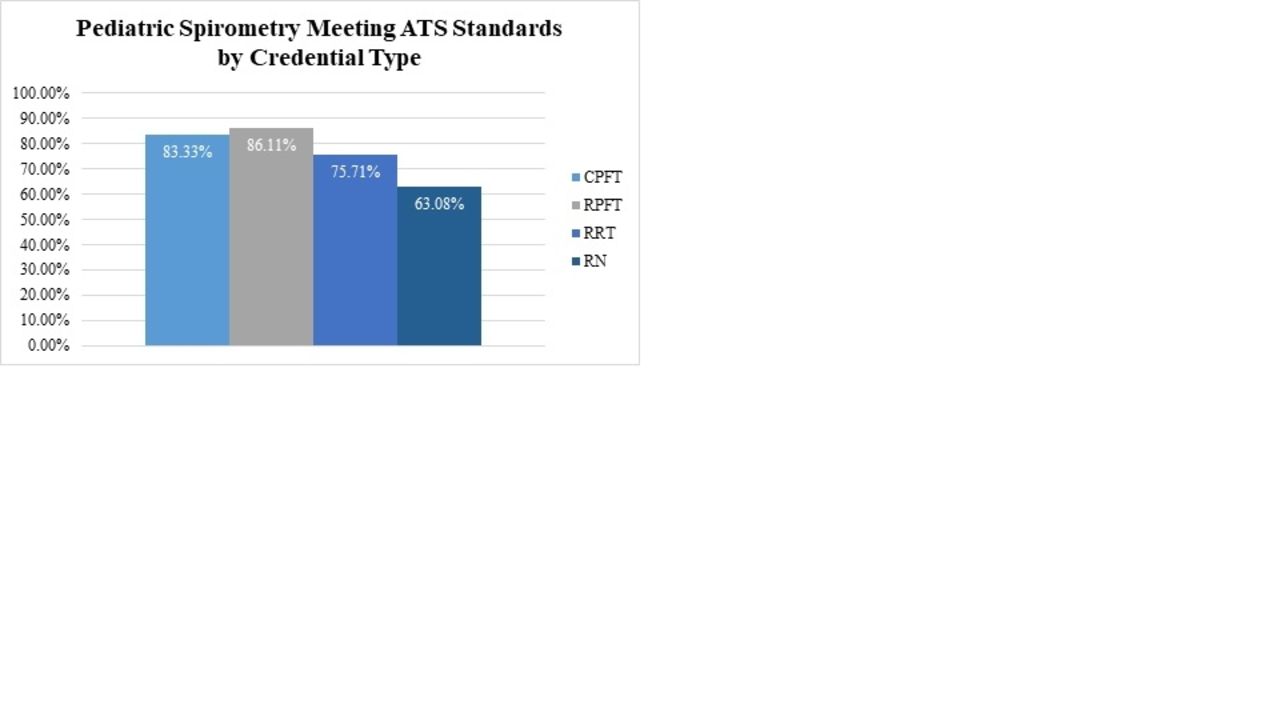
In 120 pediatric spirometry audits, patients ages were 7-19 years (average 11.2 years). When comparing RN to RT spirometry audit compliance with ATS standards we found that RNs submitted spirometry that was compliant with ATS standards 63.08% of the time. In comparison, RTs submitted compliant spirometry results 79.24% of the time. In the 60 RT audited spirometry tests 42 were done by RRTs, 6 by CPFTs and 12 by RPFTs. When comparing RT specific credentials, those with RPFT had the greatest percentage of compliance with ATS standards, followed by CPFT, then RRT (graph 1).
Conclusions:
In our pediatric hospital, compliance with ATS standards, as indicated by spirometry audits was demonstrated best by professionals with the RPFT credential. The need for extensive training and auditing should be mandated for all professionals preforming pediatric spirometry to ensure accuracy of results aligned with ATS standards. More research is needed to assess the potential impact of training and spirometry audits within the field of pediatrics. References: 1. Loeb J, et al. Acceptability and repeatability of spirometry in children using updated ATS/ERS criteria. Pediatr Pulmonol. 2008;43(10):doi:10.1002/ppul.20908 2. Pérez-Yarza E, et al. Forced spirometry in healthy preschool children. An Pediatr (Barc). 2009;70(1):doi:10.1016/j.anpedi.2008.10.003
Table 1 displays the criteria that must be met during spirometry audits in order for the spirometry to be considered in compliance with ATS standards.
Graph 1 shows the percentage of compliance with ATS standards for pediatric spirometry in our facility based on provider credential. View all access options for this article.Auditing Criteria for Acceptable Spiromtery Based on ATS Standards
ATS Criteria for an Acceptable Test
Satisfactory Start of Test:
1. Extrapolated volume < 5% of the FVC or 0.150 whichever is greater2. For children 6 and younger extrapolated volume 12.5 % of FVC or 0.080L
Satisfactory End of Test:
Performs the test with a maximum inhalation, good start, and smooth continuous exhalation with maximum effort:1. No cough in the first second2. No Valsalva maneuver3. No hesitation during the test4. No leaks5. No obstructed mouthpiece6. Plateau in the volume time curve
Acceptable and Reproducible:
1. Minimum of 3 similar loops2. Difference between the largest and the next largest FVC & FEV1 ≤ .150L 3. Patients with FVC <1.0L the difference between the largest and the next largest FVC & FEV1 ≤ 0.100L
Get full access to this article