
Abstract
Background:
Volume-targeted ventilation modes are used in NICU and neonatal transports to provide consistent and accurate tidal volume (VT) delivery so that gas exchange and lung protection can be optimized. We hypothesized there would be no differences in VT delivery in infant lung models between an ICU (Draeger VN500, Lubeck, Germany) and Transport (Hamilton T1, Reno, NV).
Methods:
The Hamilton T1 and VN500 were configured in AC-VG using standard 6 mL/kg settings for ELBW and term newborn. The Ingmar ASL 5000 ventilator was configured using a customized compliance and resistance for each model. The displayed VT on the ventilator and VT delivery to ASL were recorded both from Standby to ON for 8 breaths and following 1 minute after VT was stabilized. Mean differences between % error and bias between the ventilators were compared using T-test with significance established as P < .05.
Results:
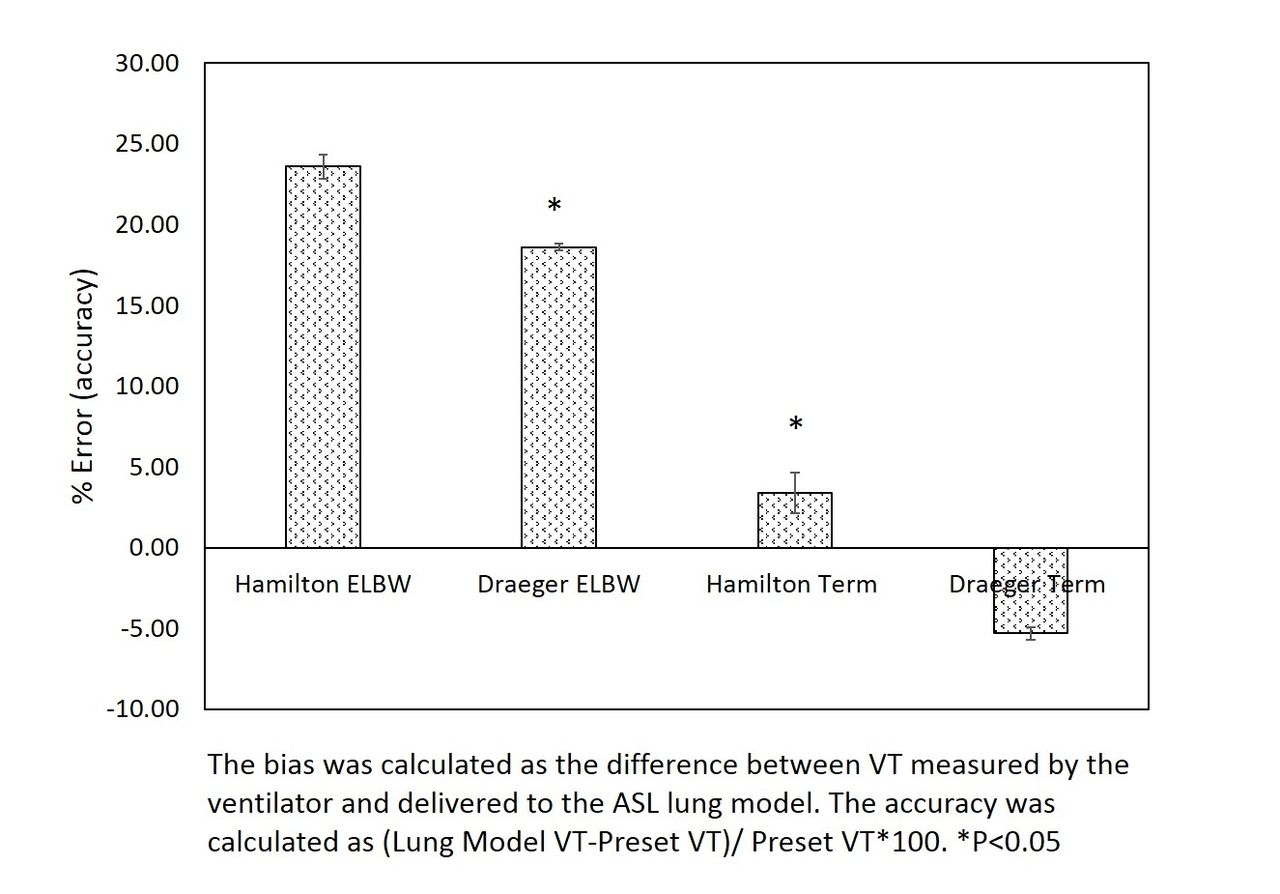
When Hamilton T100 was set to deliver VT 6 mL/kg in the ELBW model, excessive VT (∼16 mL/kg) was observed for 8-10 breaths; whereas Draeger VN remained stable with 6-7 mL/kg. The Draeger had greater accuracy than Hamilton with ELBW (P < .05) testing but was lower when compared to Hamilton with term newborn testing (P < .05). The % error was within 10% for term newborns with each ventilator. The Hamilton reported lower VT (∼2 mL) than what was delivered to the lung model, whereas Draeger VN was within 1 mL for both ELBW and term newborn.
Conclusions:
There may be important differences in VT accuracy and reported values between ICU and transport ventilators to considering when proving lung protection to infants.
Get full access to this article
View all access options for this article.