
Abstract
Background:
Hospitalized patients may present with risk factors for sleep disordered breathing (SDB) which has not been previously diagnosed or treated. Untreated SDB has been associated with increased readmission rates, poor outcomes in post ischemic stroke, and an increased risk for atrial fibrillation. In October 2015 the Respiratory Therapy and Sleep Wake Center departments collaborated with a sleep medicine physician to establish an inpatient sleep medicine program. The goal of the program was to diagnose and treat SDB during hospitalization thereby reducing the delay to treatment. Unattended sleep testing was utilized with a goal to maintain an error rate of approximately 7% which is the same rate present in our unattended home studies.
Methods:
Portable home sleep test (HST) devices were utilized to diagnose patients for SDB. Initially all night shift respiratory therapists were trained by sleep technologists to set up and place the HST equipment. After set up the therapists were instructed to check on the patient once during the night, then remove the device in the morning and deliver the device to the department. The sleep technologist would retrieve the equipment and score the study. Errors occurred when the study was unable to be scored correctly due to absence of oximetry signals, lack of detected airflow, or a poor signal from the thoracic belt. After 3 months a high error rate was noted and the process was changed in that a select team of 21 therapists and supervisors were retrained on use of the HST devices. This new training process included the use of simulated testing on coworkers. Nursing staff were also reeducated on the testing process and specific instructions were communicated via a revised order set.
Results:
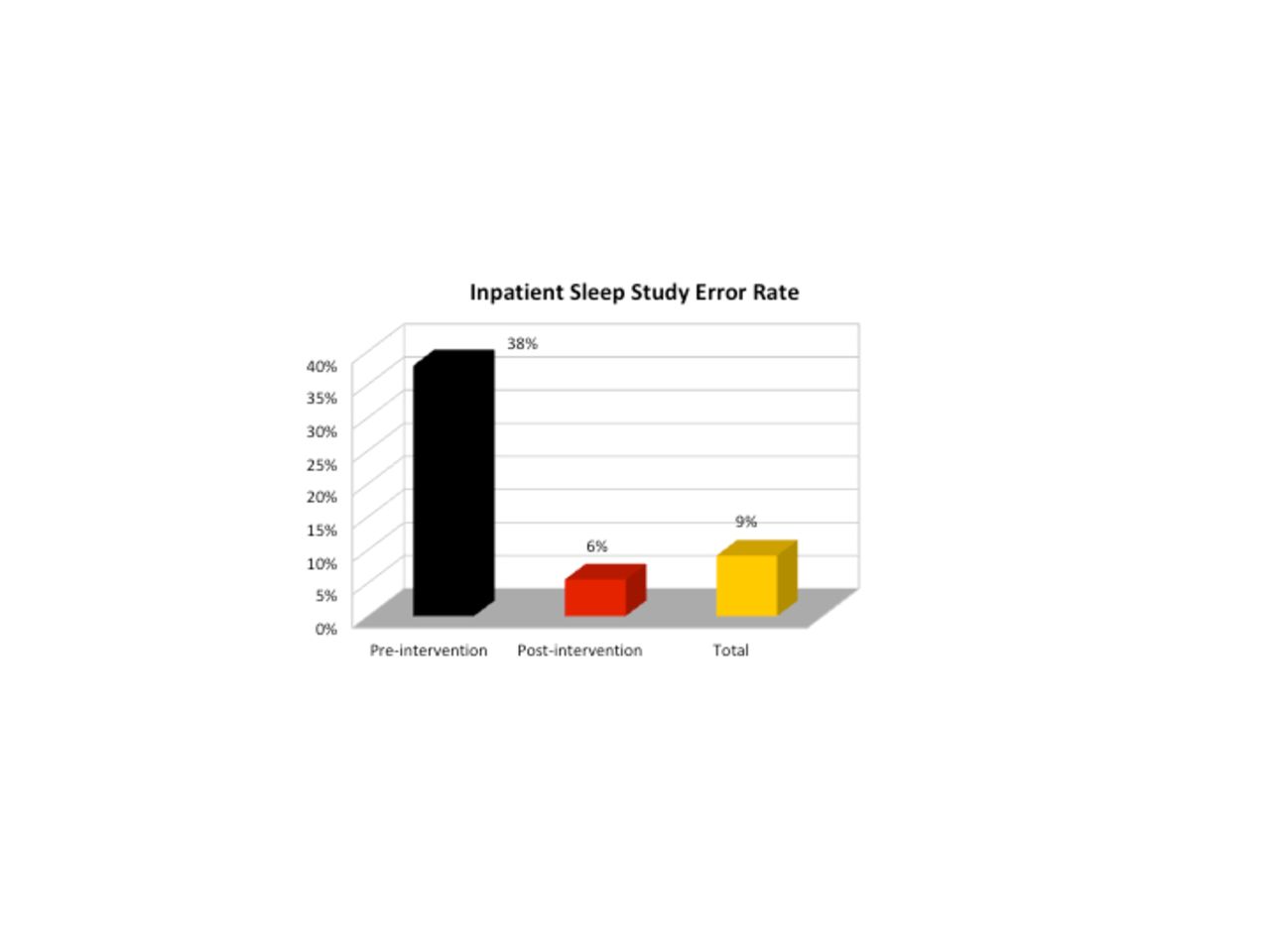
An error rate of 37.9% was present after the initial 95 studies were completed. The revised training methods were then implemented and the therapists performing studies were reduced to a core team. These changes produced an error rate of 5.5% in the subsequent 756 studies. The reduced error rate led to fewer studies that had to be repeated. As of July 2018, the total error rate was 9.2% (78/851 studies).
Conclusions:
The incidence of errors during inpatient sleep testing can be reduced through focused training, use of a core group of therapists, and improved communication. This reduction can increase the likelihood that SDB can be diagnosed and treated prior to hospital discharge. Disclosures: None
Get full access to this article
View all access options for this article.