
Abstract
Background:
A tertiary hospital in central Taiwan began to implement VAP Bundle Care in 2011, initially with 1. maintaining head of bed at 30-45 degrees, 2. daily extubation assessment, 3. whether using antacids, 4. daily oral care using 0.12%-0.2% chlorhexidine, 5. Cuff pressure 20-25 cm H2O five items for implementation, from July 2015, the Infection Control Society of Taiwan requested to change to 1. Ventilator liberation evaluation, 2. daily interruption of sedatives, 3. daily oral care using 0.12%-0.2% chlorhexidine 4 maintaining head of bed at 30-45 degrees 5. draining of ventilator circuit, so this study discusses the impact of such changes on clinical infection control.
Methods:
This study retrospectively collected the number of cases of pneumonia infected and the infection rate (thousands of people) in seven intensive care units collected by the hospital's infection control team from 2013 to 2017, and divided the collected data into 30 months each. Comparing the two groups, the experimental group was from July 2015 to December 2017, and the control group was from January 2013 to June 2015, with narrative statistics, F-test and t-test for statistical analysis.
Results:
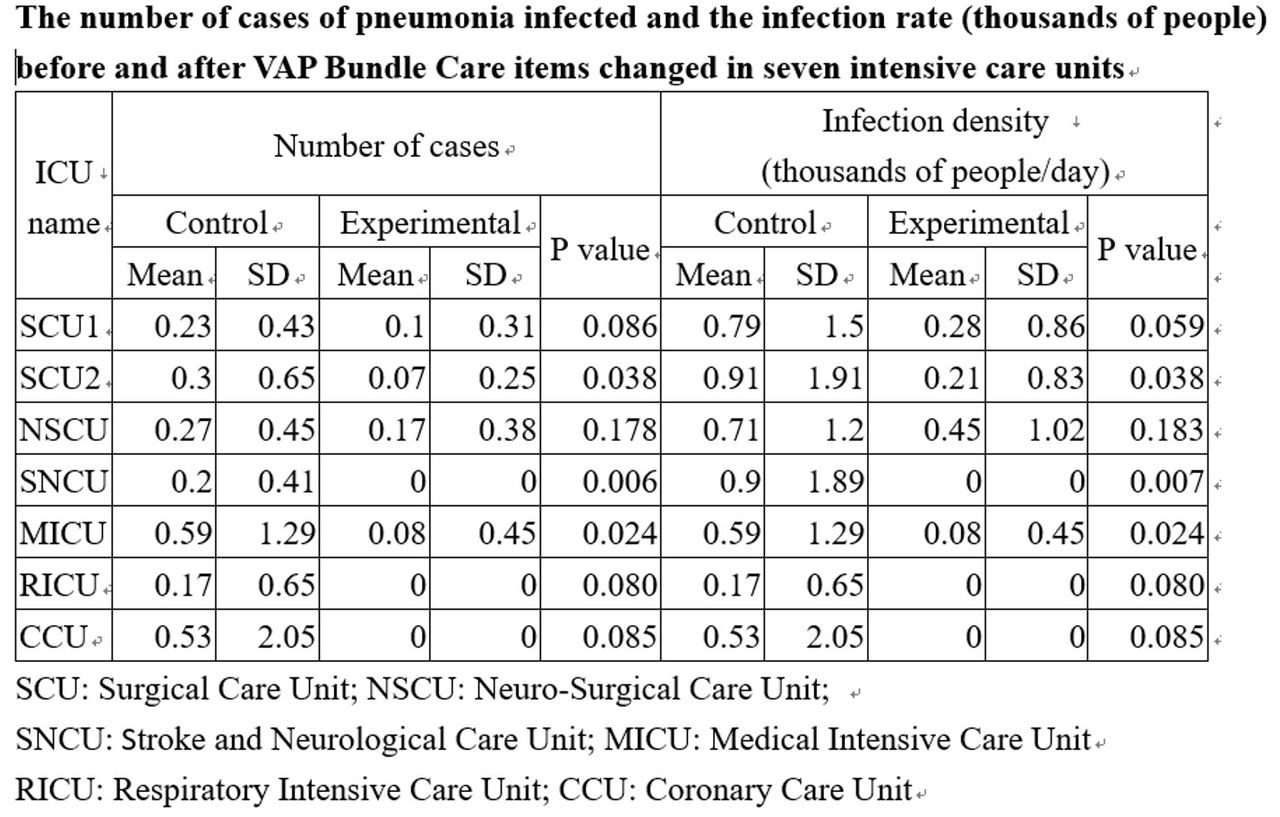
According to the results of the study, daily extubation assessment, whether using antacids and Cuff pressure 20-25 cm H2O were changed to the ventilator liberation evaluation, daily interruption of sedatives and draining of ventilator circuit will be stopped. The number of patients infected with pneumonia and the infection rate (thousands of days) were not significant in the surgical intensive care unit (SCU1 and NSCU) and the intensive care unit (RICU and CCU) (P >0.05), in the surgical intensive care unit (SCU2 and SNCU) and Internal Medicine Intensive Care Unit (MICU) were significantly (P < .05) (see table).
Conclusions:
Changing the implementation items of VAP Bundle Care, the number of cases of pneumonia infected by patients using ventilators and the infection rate were not significant in the four intensive care units, indicating that such changes would not affect the clinical infection, but there were 3 intensive care units in the implementation of the project after the change, the ward infection rate also decreased, and its possible influencing factors deserve further management discussion.
Get full access to this article
View all access options for this article.