
Abstract
Background:
Ventilator-induced lung injury is precipitated by the non-physiological distribution of tidal volume in the lungs, increasing the pressure exerted on alveoli that receive greater volume, and causing the eventual collapse of alveoli that do not receive enough tidal volume. Electrophrenic transvenous neurostimulation respiration (ETNR) stimulates a diaphragm contraction, in synchrony with the ventilator, and may address this problem by re-distributing tidal volume in a more physiological pattern and keeping the lungs open. More alveoli are thus available to receive tidal volume, improving dynamic compliance and reducing ventilation pressures.
Methods:
A pilot study was conducted using a large animal model (50 kg pigs) mechanically ventilated in a mock intensive care unit. Subjects were deeply sedated and subjected to lung-protective ventilation at 8 mL/kg in volume control. ENTR, selectively adjusted to reduce ventilator pressure-time-product by 15-20%, was delivered every second breath, in synchrony with the inspiratory phase of ventilator-triggered breaths. Peak inspiratory pressure (PIP) and dynamic compliance (Cdyn) were recorded at the start of study and values for MV breaths (no diaphragm contraction) were compared to MVP breaths (ETNR diaphragm contraction) within 5 minutes of each other. Means were compared by paired t-test with a significance level of alpha of 0.5 and beta of 0.80. Institutional Review Board permission was granted for this study.
Results:
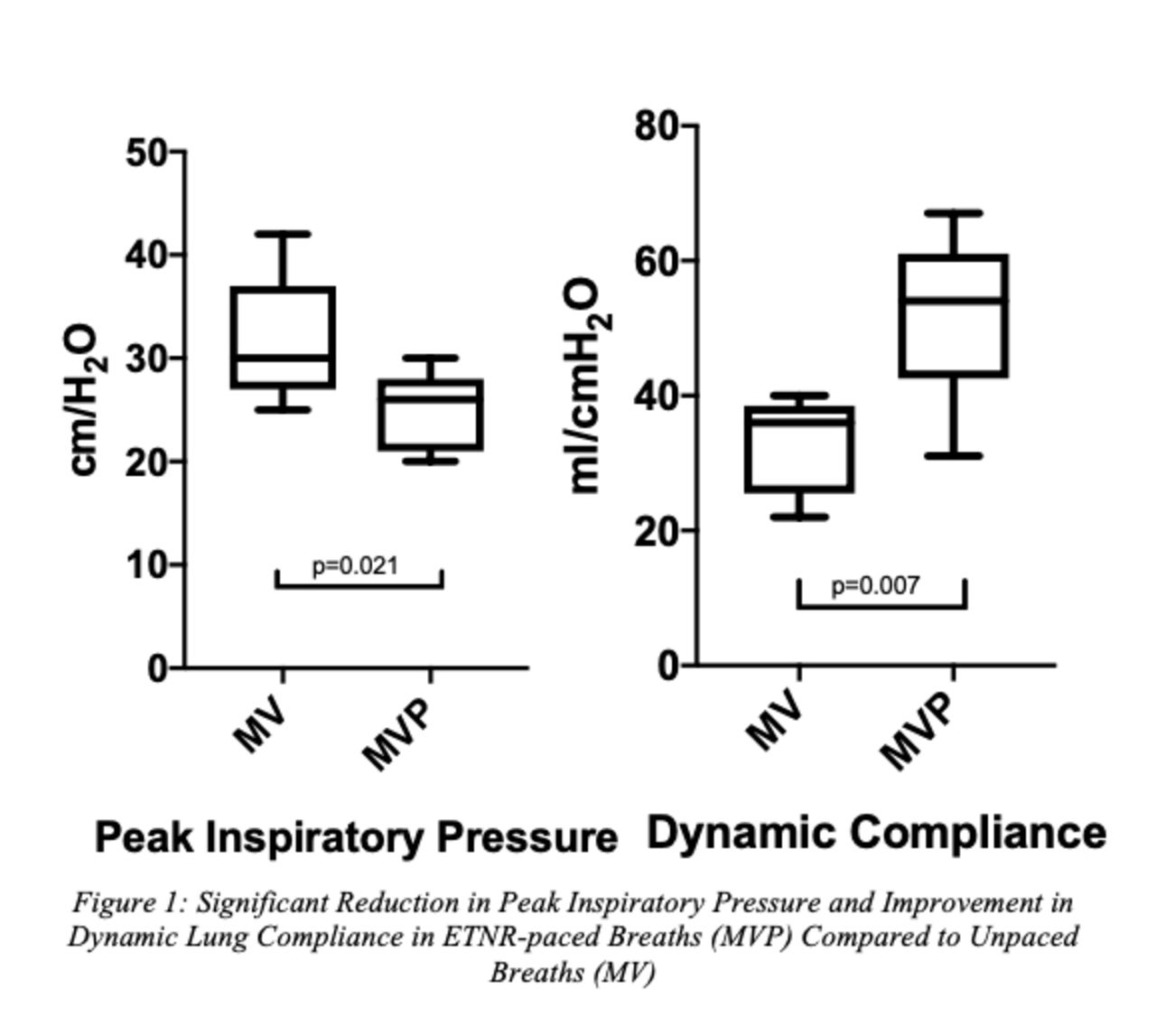
PIP significantly dropped 21%, from 31.6 cm H2O in MV breaths to 24.8 cm H2O in MVP breaths with the addition of ETNR diaphragm contraction during inspiration (P = .021). Cdyn significantly improved 59%, from 32.8 mL/cm H2O in MV breaths to 52.2 mL/cm H2O in MVP breaths with the addition of ETNR diaphragm contraction (P = .007).
Conclusions:
ETNR diaphragm contraction used as an adjunct to mechanical ventilation significantly decreased PIP and improved Cdyn at the selected intensity. This is an important finding, as a reduction in inspiratory pressure translates into less ventilator-induced lung injury and better outcomes in the ICU. This technology has the potential to provide a novel method of lung-protective ventilation in sedated, ventilated patients. Disclosures: Study sponsorship, technical support and equipment provided by Lungpacer Medical. PhD student salary funding provided by a grant from Lungpacer Medical and Mitacs. Dr. Reynolds is a paid consultant with Lungpacer Medical.
Get full access to this article
View all access options for this article.