
Abstract
Background:
Maintaining a busy assignment can make it difficult for RTs to attend patient rounds and provide feedback, administer and evaluate treatment response, and still be able to maintain a safe clinical environment for patients. Historically, RTs perform ventilator and noninvasive device checks every 2-4 hours in most children’s hospitals. Reducing the amount of time RTs spend charting device checks may allow more focused bedside care. The specific aim of this project was to determine whether improvements in workflow could allow RTs more time to attend rounds and to provide other value-added work without sacrificing patient safety.
Methods:
A committee of RTs reviewed the published literature, current RT workflow, and developed a survey to assess reasons why they were unable to attend rounds, and preferred device check/patient assessment frequency. Based on survey data, a policy was developed to determine frequency for device checks and patient assessments based on RT preference. We tracked NICU safety events (e.g. unplanned extubations, nasal pressure injuries, etc) as well as RTs’ ability to attend NICU rounds prior to and following RT workflow changes.
Results:
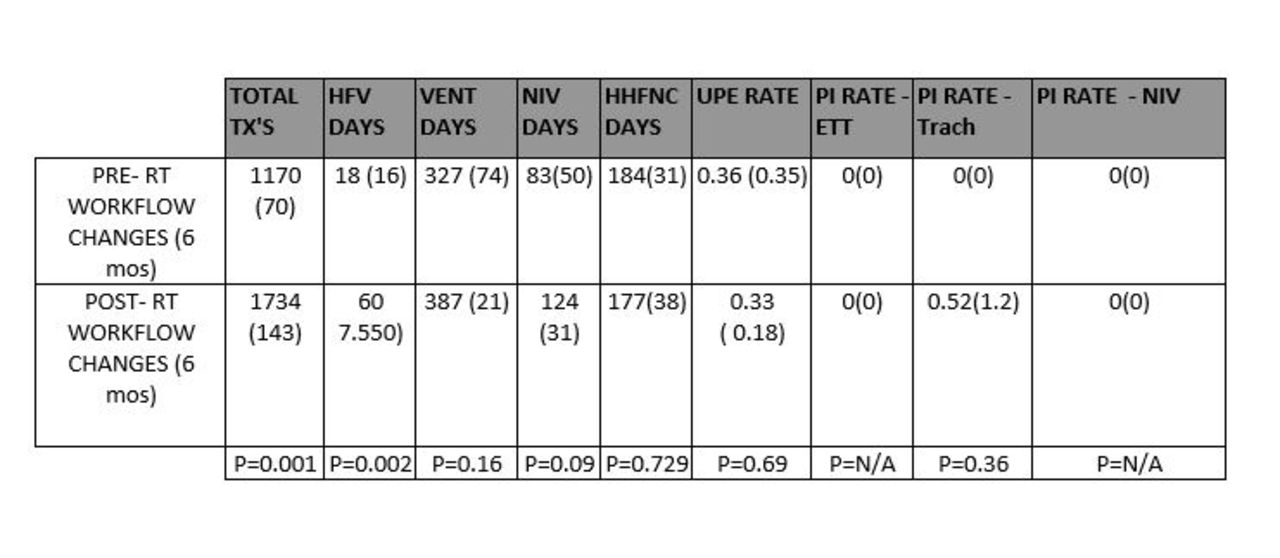
The majority of RTs preferred twice per shift (46%), followed by Q4 (33%), and Q shift (31%) device checks. Device checks were changed from Q4 to twice per shift with patient assessments in between. The total number of NICU RT treatments increased by 148% after implementing these workflow changes (P < .001, Table 1). However, RTs’ ability to attend daily patient rounds increased from 65.5% (6 months) to 81% (30 days) between the pre to post workflow periods, respectively. There were no observed differences in unplanned extubations, or pressure injury rates related to the increased workload (Txs and HFV, Table 1) or changes in workflow.
Conclusions:
Currently, there is no national guideline that suggests optimal frequency for device checks in NICUs. The AARC suggests that patient-ventilator assessment intervals be institution-specific. We demonstrated a short-term increase in the NICU RTs’ ability to attend patient rounds by following a process that allowed RTs to establish their own workflow. We did not anticipate the large combined increases in workload based on NICU treatments or ventilator/NIV days. We believe that workflow changes allowed RTs the ability to spend less time charting and more time contributing to value-added care without increasing risk for complications.
Get full access to this article
View all access options for this article.