
Abstract
Background:
To provide a consistent clinical practice and timely interventions in the management of our cardiothoracic surgical patients who require mechanical ventilation post operatively. We updated our policy regarding the care of this specialized patient population with a focus on improving the timeliness of the weaning and extubation process. Utilizing our “Cardiac Fast Track Weaning” pathway, we proposed that the Respiratory Therapist would perform a ventilator check at least every 30 minutes for the first two hours to assess readiness for extubation.
Methods:
Cardiac Fast Track Weaning order was placed in the EMR as a part of the post-operative order set by the surgeons. Patients were identified as a Fast Track candidate during ECHO report immediately upon arrival to the ICU. The Respiratory Therapist utilized the CVICU Fast Track Weaning Flowchart as a guide to assess patient for readiness, with a goal to extubate the patient safely within four hours upon arrival to the ICU. The Respiratory Therapist assessed the patient and monitored the ventilator immediately after initiating mechanical ventilation, at least every 30 minutes for the first 2 hours, and then at 2 hour intervals thereafter. Once patient met the eligibility requirements the patient was placed on pressure support, with a goal of tidal volume at least 6-8cc/kg IBW. If the patient met the extubation criteria as determined by the pathway, the Respiratory therapist would notify the physician the patient was ready for extubation.
Results:
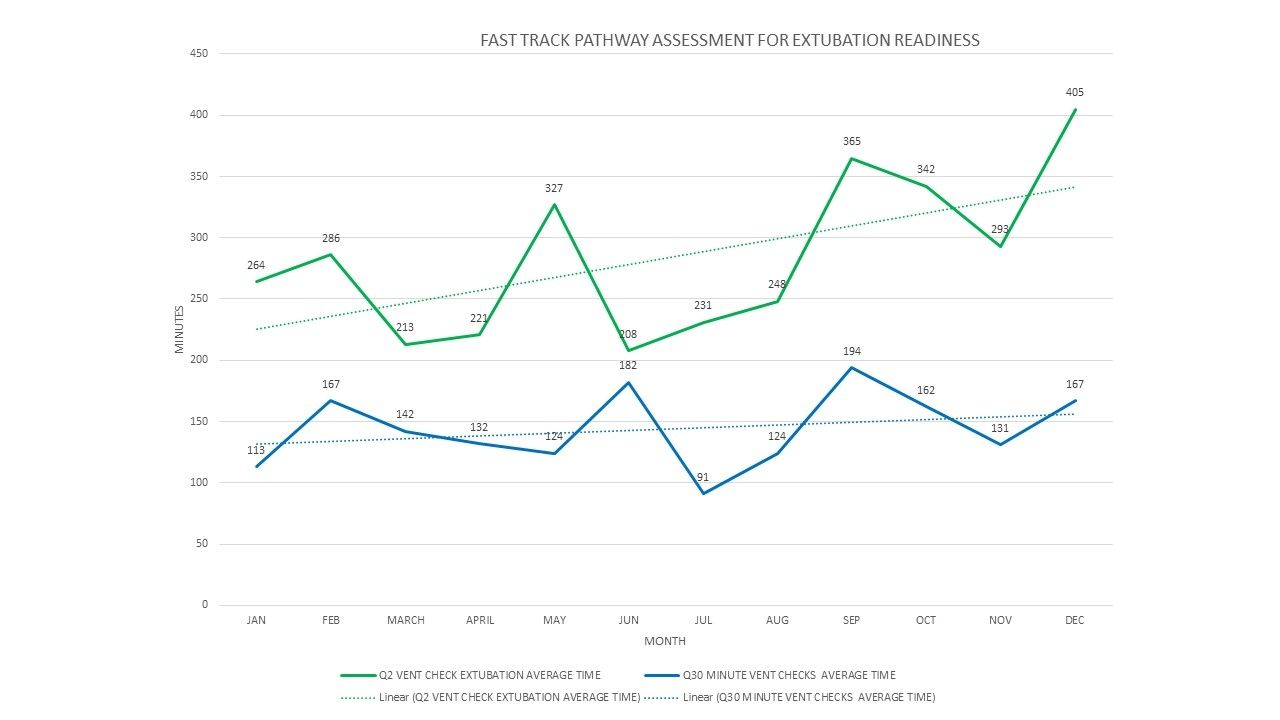
Data collected from January 2018 to December 2018 showed a decrease in extubation time. Patients identified as Fast Track had an average of 144 minutes, compared to 284 minutes with patients who did not receive the Q30 minute assessment.
Conclusions:
When the pathway was followed with patient and ventilator assessments every 30 minutes, time spent on the ventilator was significantly lower.
Get full access to this article
View all access options for this article.