
Abstract
Background:
In many facilities, billing is directly connected to patient medical records and documentation. Unfortunately, the relationship between these two entities leave a lot of room for error. These errors can result in under and over charging of patients due to incorrect documentation, errors in coding, and poor interoperability between documentation and billing systems. This study looks specifically at errors of missing ventilator, BiPAP, or CPAP documentation and its effects on patient billing.
Methods:
For the purposes of this study, data related to documentation and billing was collected for one month. To find patients with missed documentation a report was pulled from a hospital worklist that showed all patients receiving respiratory treatment in the facility. The report was then reduced to show only ventilators, BiPAP, and CPAP tasks. This report was kept until the following day and was then manually cross referenced against charges from the day before. All patients then identified as having a task, but no charge from the previous day were further investigated by looking into the clinician documentation. After investigation of documentation all patients that were found to have missing documentation associated with charges were recorded and the correct charge entered into the patient’s charts. Data was then tallied on a daily basis to assign a dollar amount associated with what would have been losses in revenue.
Results:
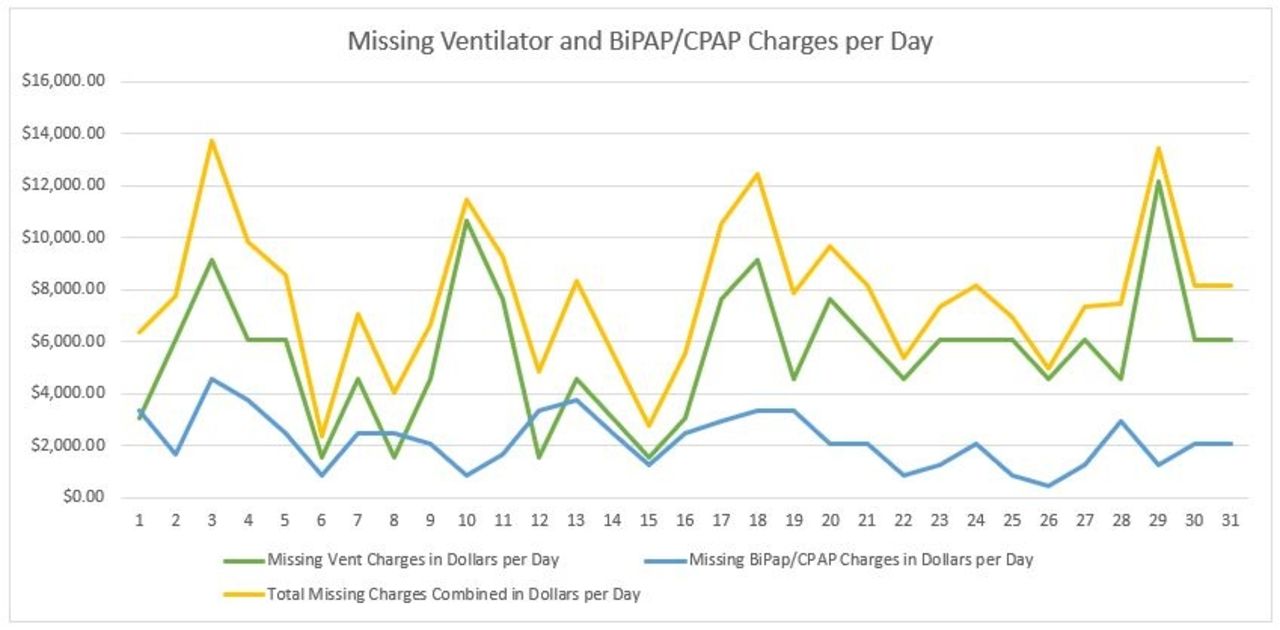
After one month it was found that the facility we looked at was missing approximately 3.8 ventilator and 5.1 BiPAP or CPAP charges a day. According to our findings, the mean ventilator charge in a hospital setting is about $1,522 per day, and a BiPAP or CPAP is approx. $416.10 per day. Using those figures, we were able to determine that without auditing there was a potential loss of ventilator revenue amounting to $5729.88 per day. Loses from missing BiPAP and CPAP charges would account for an additional $2,117.21 per day. That is an estimated loss of revenue of $7,847.10 per day from just ventilator, BiPAP, and CPAP documentation errors alone.
Conclusions:
In conclusion, documentation in the healthcare setting is extremely important for many reasons. Not only does it act as a record for history of treatment and prior visits, but in today’s time is often responsible for the billing of treatment and care. In this study alone, the auditing and correction of documentation and charges could have saved an estimated $2,864,155 in missed revenue.
Get full access to this article
View all access options for this article.