
Abstract
Background:
Utilization of invasive ventilation can lead to adverse events or hospital-acquired conditions for the neonatal patient such as long-term damage to the lungs, increased risk of infection, ventilator-associated events, and unplanned extubations. Implementation of a respiratory therapist (RT) driven protocol can safely standardize ventilator weaning strategies in post-operative neonatal patients, thereby reducing associated risks to patients.
Methods:
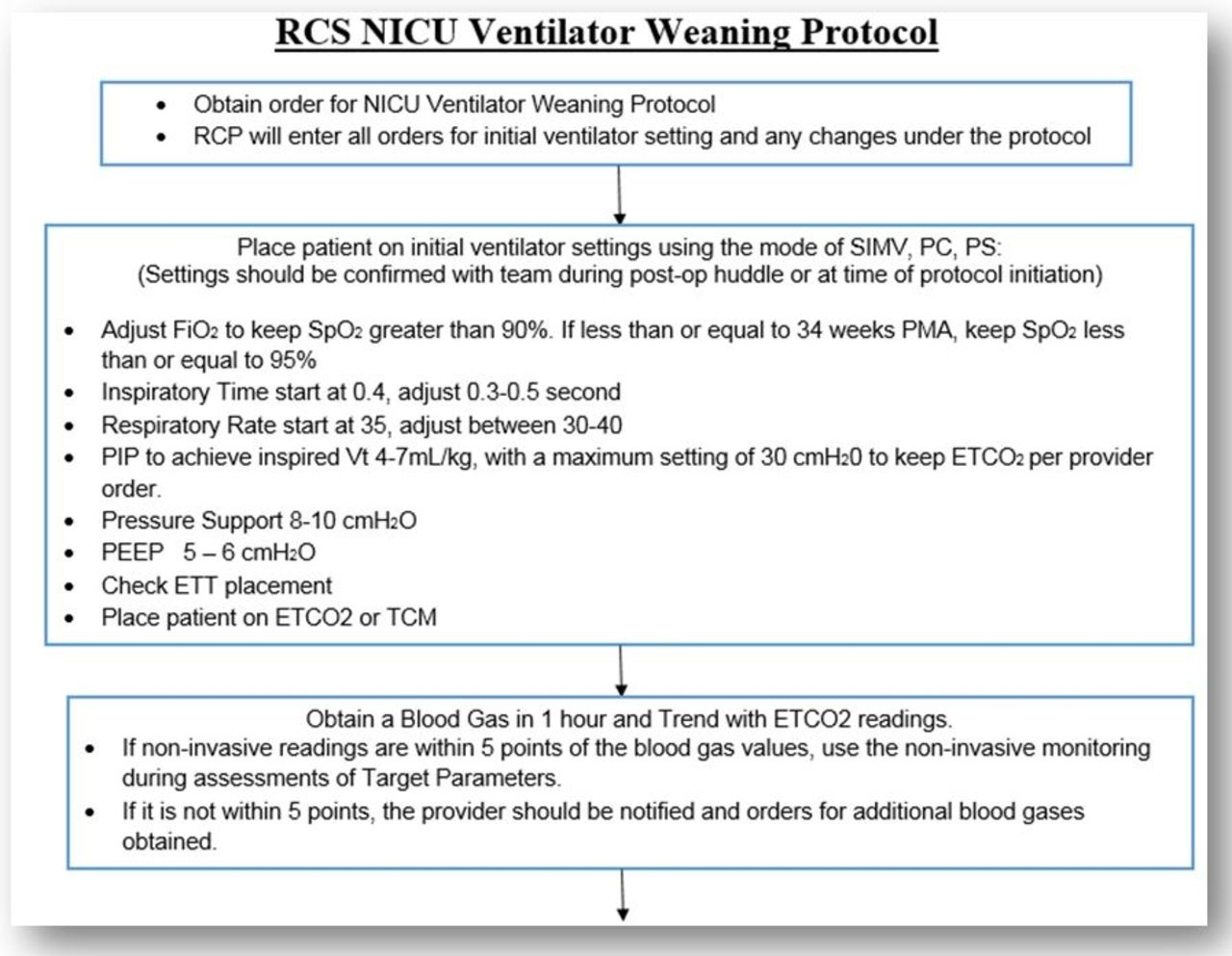
An RT driven protocol was developed, allowing the RT to manage the weaning of post-operative patients within the Neonatal Intensive Care Unit (NICU). Post-op patients greater than 2 kg were included if they did not receive blood products in surgery. Patients with pulmonary or airway comorbidities potentially impacting extubation success were excluded. The implementation of the protocol required a provider order. The Institutional Review Board approved this protocol. Real-time data was collected on patients admitted post-operatively to the NICU from November 1, 2016 to April 2, 2017. The NICU Post-op Ventilator Weaning Protocol was initiated on April 3, 2017. On December 3, 2019 the protocol was updated to be more inclusive; expanded to all invasively ventilated patients with postmenstrual age of greater than 29 weeks, and eliminated post-operative and weight requirements.
Results:
During the 6-month pre-data collection period, 5 patients were identified as fitting the protocol requirements. Mean weight was 2.69 kg, ranging from 2.44 to 2.84 kg. Average time to extubation was 17.8 hours, ranging from 7 hours to 23.75 hours. During the first two years, 33 patients were ordered for the NICU Ventilator Post-op Weaning Protocol. Of these, 5 patients were removed due to provider preference and 1 patient was removed due to multiple failed weaning attempts. There were 27 patients who successfully completed the protocol to extubation. Mean weight was 2.78 kg, ranging from 1.75 to 4.04 kg. The average time to extubation decreased slightly from the pre-data sample to 17.5 hours, ranging from 1.08 hours to 54.5 hours. Only one patient was reintubated within 24 hours of extubation due to stridor. No adverse events were reported.
Conclusions:
Implementation of a RT driven ventilator weaning protocol allows the RT to expand their scope of care and safely standardize the ventilator weaning process. Additionally, increasing the autonomy of the RT at the bedside, improved both RT staff and provider satisfaction
Get full access to this article
View all access options for this article.