
Abstract
Background:
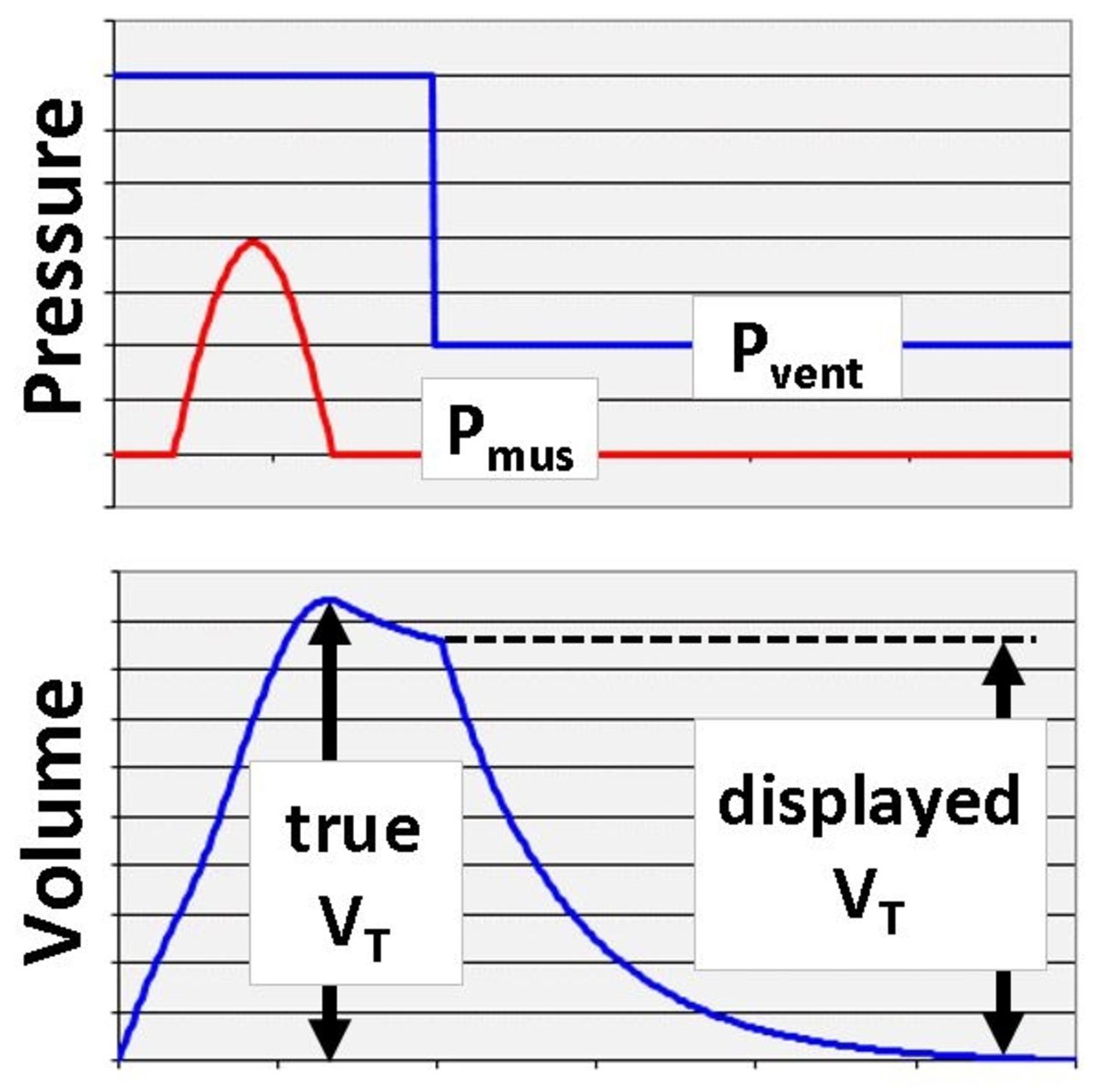
Studies confirm that excessive tidal volume (VT) increases the risk of ventilator induced lung injury. A previous model study by Chatburn et al (Comput Biol Med 2016;75:235-242) showed that VT measurement error may occur during pressure control ventilation (PCV) with preset inspiratory time (TI). Some ventilators calculate VT as integral of flow over TI or expiratory time (TE). For a passive patient during PCV, this calculation is accurate. However, an inspiratory effort increase then relaxation results in expiratory flow during TI. Integration of expiratory flow results in volume deducted from the calculated VT (see figure). Hence the displayed volume is lower than the peak value of the volume waveform, the true VT. The displayed VT will be inaccurately low, possibly leading to inadvertent tidal volume over-dosage. The purpose of this study was to determine the prevalence of two main outcome variables: VT error and VT over-dosage (ie, VT >8 mL/kg) during routine mechanical ventilation with PCV modes in our ICUs.
Methods:
All patients in medical and neuro ICUs with active inspiratory efforts, in PCV modes, using Medtronics PB840 or GE Carescape R860 ventilators were included. Volume (V) waveforms were observed for at least 10 breaths per patient. Waveforms with downward V deflection (see figure) during TI were deemed to have VT error present. If error was present, error size was calculated by subtracting the digital display of VT from the peak value of the V waveform.
Results:
We recorded data for 50 patients. A VT error was present in 32% of patients. Average error was -1.2 mL/kg (range -0.6 to -2.6). However, 75% of the time the error was too small to calculate. VT over-dosage occurred in one patient whose displayed VT was 7.9 mL/kg but true VT was 10.4 mL/kg. This patient also had the longest TI (1.2 s).
Conclusions:
In this small pilot study, we observed that VT error is present in a substantial portion of patients during PCV, with the largest error being associated with the longest TI as expected from the previous study. Results of this study warrant the need to monitor V waveforms for patients receiving PCV with an active exhalation valve feature to ensure patients are receiving VT in the range of 6-8 mL/kg of ideal body weight
Get full access to this article
View all access options for this article.