
Abstract
Background:
There is limited evidence supporting an optimal method or frequency for suctioning hospitalized infants with bronchiolitis. This study was designed to evaluate short-term physiologic outcomes between nasal aspiration and nasopharyngeal suctioning in this population.
Methods:
Sixteen infants requiring hospitalization for supportive management of bronchiolitis were instrumented with transcutaneous carbon dioxide (TcCO2) and oxygen (SpO2) monitors. Global and regional changes in inspiratory and end-expiratory lung volumes were recorded with electrical impedance tomography (EIT). Subjects were suctioned with both nasal aspiration and nasopharyngeal suctioning methods in a randomized order. Noninvasive gas exchange and lung volumes were measured at baseline (pre-suction) and at 10, 20, and 30 minutes following each suctioning intervention. Pre-and-post clinical respiratory severity scores and sputum mass were obtained with each suctioning epoch.
Results:
There were no differences in SpO2 (P = .88), TcCO2 (P = .41), heart rate (P = .31), breathing frequency (P = .15), inspiratory lung volumes (P = .93) or delta end-expiratory lung volumes (P = .53) over the course of suctioning between nasal aspiration and nasopharyngeal suctioning. Figure 1A and 1B show inspiratory lung volumes and delta end-expiratory lung volumes, respectively. The sputum mass was approximately 33% greater with nasopharyngeal but sputum mass (P = .14) and clinical respiratory score pre-post suctioning (P = .97) were not different between the two suctioning interventions. Sputum mass was not associated with delta end-expiratory lung volumes at 30 minutes for nasal aspiration (ρ = 0.11, P = .69), but had a moderate association for nasopharyngeal suctioning (ρ = 0.048, P = .048).
Conclusions:
Infants with viral bronchiolitis appeared to tolerate both techniques without any increased short-term risk in signs of clinical deterioration, gas exchange, lung volumes or adverse events following sputum removal. These findings may help aid clinicians in selecting appropriate suctioning techniques in infants with viral bronchiolitis. It is possible that a subset of patients may benefit from one type of suctioning over another. Future research focusing on important outcomes with suctioning patients with bronchiolitis with varying degrees of lung disease severity is needed.
Figure 1A values represent weight adjusted, global inspiratory lung volumes (arbitrary units/kilograms) and Figure 1B values show weight adjusted, global delta end-expiratory lung volumes (arbitrary units/kilograms) at baseline and at three time points (10, 20, 30 minutes) following nasal aspiration and nasopharyngeal suctioning. The median is the middle line inside the box with the mean designated as either a circle or + sign inside the box.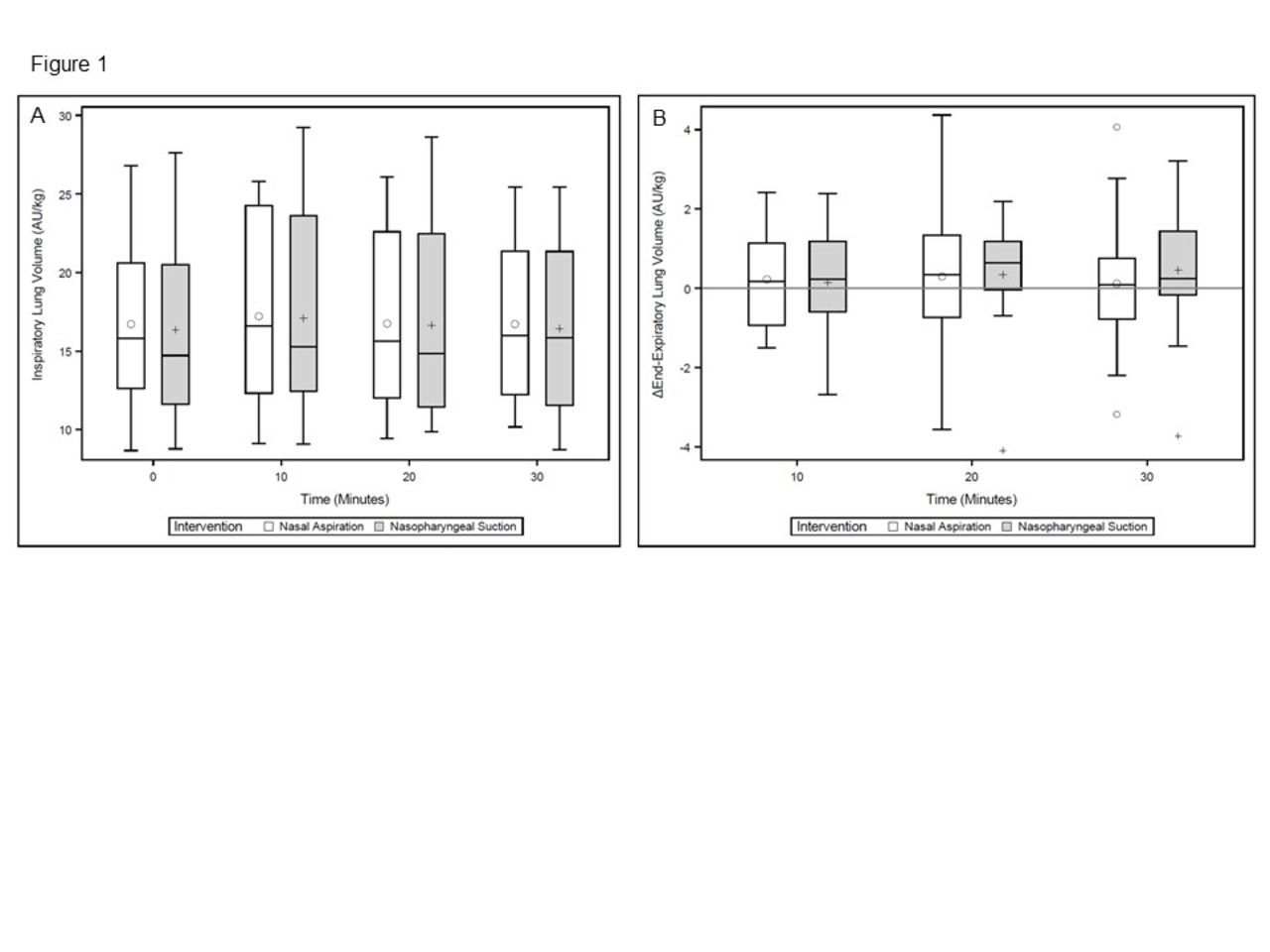
Get full access to this article
View all access options for this article.