
Abstract
Background:
Noninvasive ventilation (NIV) and high-flow nasal cannula (HFNC) are extensively applied to prevent extubation failure. The advantages of HFNC include stable oxygen supply and positive end expiratory pressure effect have been demonstrated in patients with heart failure to reduce right heart preload and relieve dyspnea. We aimed to compare the effectiveness of HFNC with NIV for preventing extubation failure in critical ill patients with heart failure.
Methods:
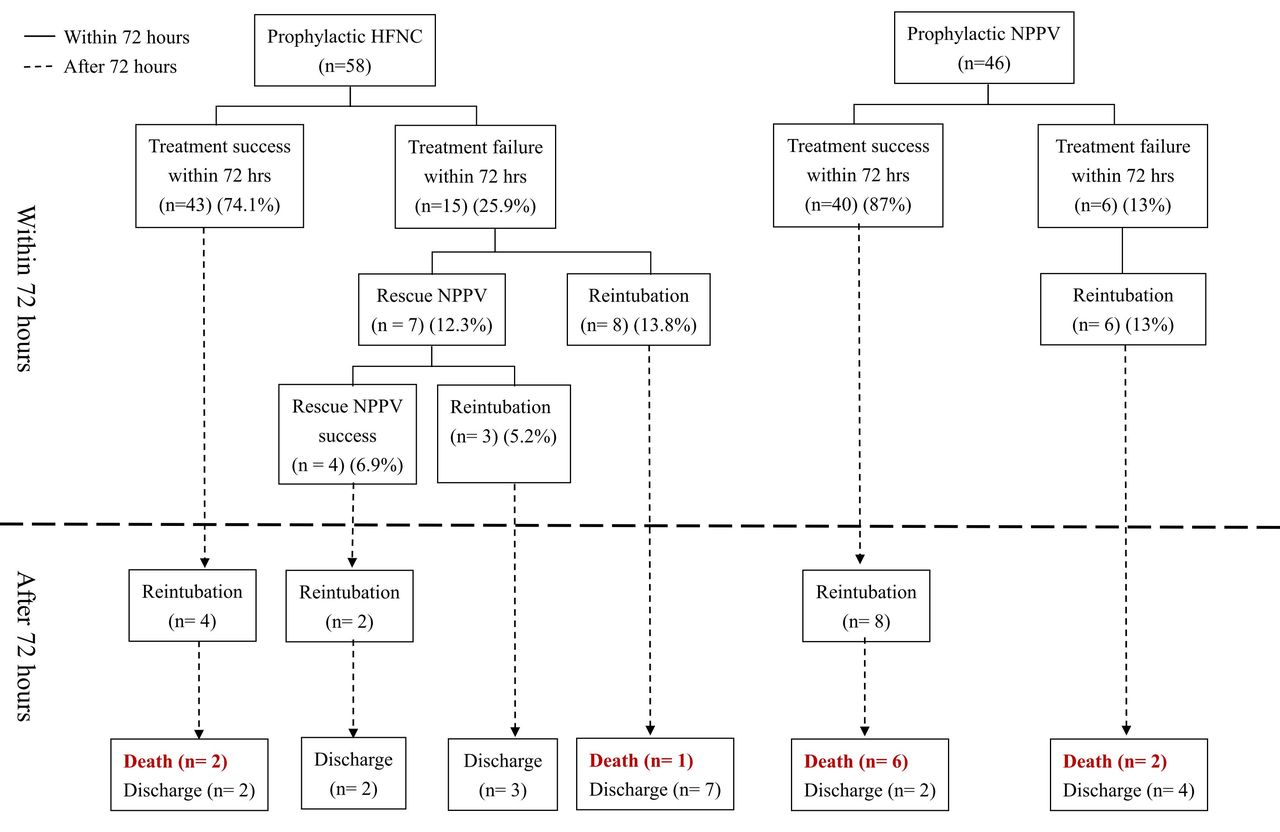
This was a three-year retrospective and single-center study approved by the ethics committee of Taipei Medical University. A total of 104 patients with heart failure (Left ventricular ejection fraction less than 50%) who were treated with prophylactic HFNC and NIV after extubation were included. Patients who refused reintubation were excluded. Clinical data including demographics, comorbidities, echocardiographic data and weaning parameters were collected. The primary outcome was treatment failure within 72 hours. Treatment failure was defined in the HFNC cohort as escalation to NIV or reintubation, and it was defined in the NIV cohort as requiring reintubation. Secondary outcomes were reintubation, intensive care unit (ICU) and hospital lengths of stay (LOS), and hospital mortality. Chi-square, Fisher exact and Mann-Whitney U test were used to compare variables between two cohorts. We performed two multivariate logistic regression analyses including clinical variables associated treatment failure and hospital mortality, with a P value < .2 using univariate analysis.
Results:
Treatment failure within 72 hours was no significant difference between the two cohorts (P = .106). Hypoxemia respiratory failure was significantly lower in NIV (P = .031). Hospital mortality was significantly lower in HFNC cohort (P = .044). No significant differences were found in reintubation, ICU and hospital LOS. The multivariate logistic regression model revealed that NIV as prophylactic treatment and reintubation were independently associated with hospital mortality.
Conclusions:
In patients with heart failure, the effectiveness of prophylactic HFNC in preventing extubation failure is similar to NIV. However, prophylactic HFNC resulted in lower hospital mortality. We suggest that HFNC can be routinely applied after extubation, but selective patients may need NIV. Disclosures: All authors conflict of interest: none. All research funding, sponsorships, provision of equipment, or other financial support: none
Get full access to this article
View all access options for this article.