
Abstract
Background:
A significant and unexplainable increase in ventilator-associated events (VAE) was noted in the ICU’s of Penn Medicine Lancaster General Hospital. An interdisciplinary team was formed, and LEAN A3 problem solving techniques were used to try and reduce VAEs. Multiple PDCA cycles were used to improve compliance with ventilator bundles. After compliance was verified, it was discovered that many VAEs were potentially avoidable and could be attributed to PEEP and/or FIO2 not being returned to baseline after a hypoxic event had resolved. We hypothesized that daily monitoring of ventilator settings could help to reduce unnecessary Ventilator-Associated Conditions (VAC); therefore, reducing Infection-Related Ventilator-Associated Complications (IVAC) and Possible Ventilator Associated Pneumonia (PVAP) as well.
Methods:
In December 2018, a standardized approach to monitor for VAE was implemented, and used a tool in the EMR that recorded the daily minimum settings for PEEP and FIO2. Frequent, preferably daily, audits of the ventilator settings compared baseline settings to current settings. If patients were at risk for “flagging” as a VAC, discussions of the current ventilator settings and plan of care occurred with the ICU care team at the bedside. Attempts to wean the PEEP and/or FIO2 back to baseline occurred if it was clinically indicated and appropriate for the patient.
Results:
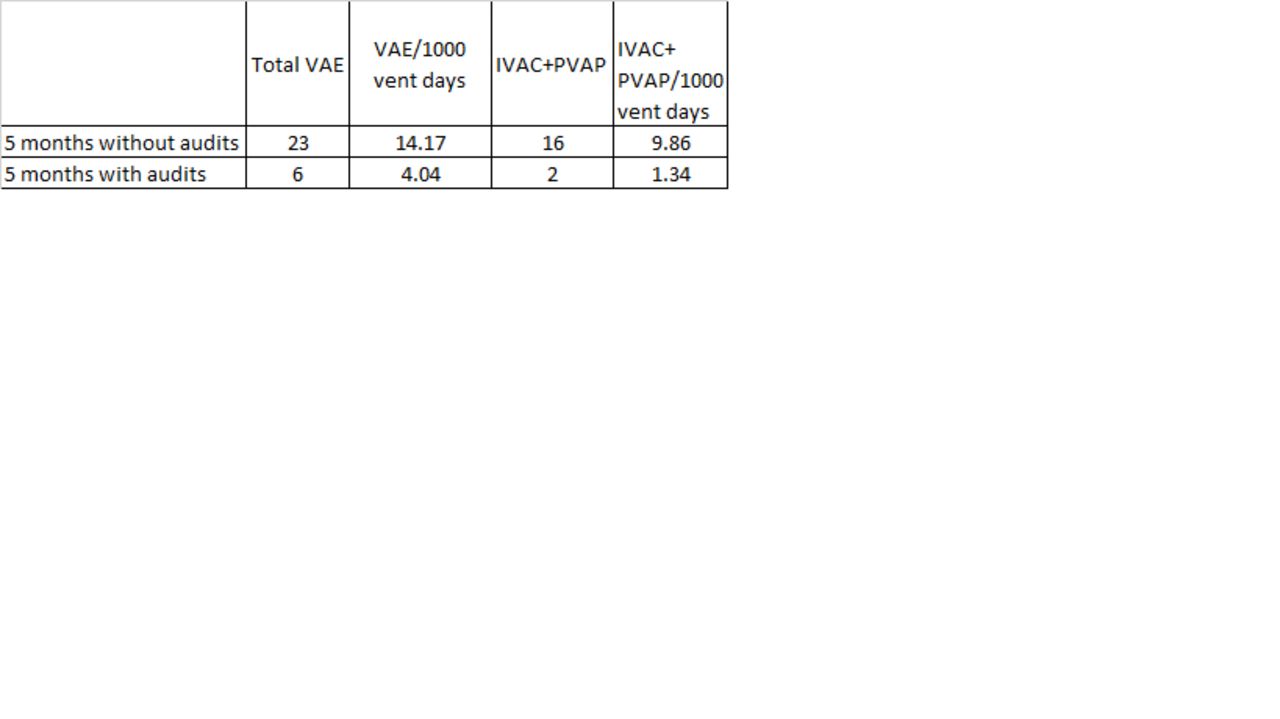
In the 5 months prior to auditing, 23 VAE (14.17 VAE/1000 vent days) were observed. During the five months after auditing implementation, 6 VAE (4.04 VAE/1000 vent days) were observed. Infections (IVAC + PVAP) decreased from 16 (9.86/1000 vent days) without audits to 2 (1.34/1000 vent days) with audits during the same respective time periods. During the experimental period, a significant reduction in overall VAE were noted [P = .001].
Conclusions:
Standardized monitoring of ventilator settings can play a role in reducing overall VAE. Referred to as weaning with a goal, weaning of the PEEP and FIO2 contributed to this reduction due to known preferable/baseline ventilator settings. Patient safety and appropriate treatment must still remain a priority in this process. Lack of knowledge about VAE guidelines was a barrier that was overcome through real-time education at the bedside. Our next step will be to continue this process to determine if these results are sustainable.
Get full access to this article
View all access options for this article.