
Abstract
Background:
Preterm neonates (gestational age< 32 weeks) often need respiratory assistance in the delivery room (DR) and during transport to the Neonatal Intensive Care Unit (NICU). As part of a quality improvement (QI) project evaluating initial interventions for preterm infants, it was identified that the time to establish respiratory support upon arrival to the NICU was a barrier to completing the required care within the first hour of life. The DR team was challenged to improve team workflow and develop an apparatus that allowed for resuscitation and initiation of invasive or nasal noninvasive (NIV) respiratory support in the DR, thus decreasing time spent initiating such support in the NICU. Given that respiratory support is always placed prior to umbilical line (UL) placement, the start time of UL placement was used as a measure of completion of respiratory support establishment in the NICU. Goal: To decrease the time from NICU arrival to start of UL placement by 20% over a period of 5 months.
Methods:
QI data collected for preterm deliveries was examined at two points: 1.) Time in minutes from birth to arrival in the NICU 2.) Time in minutes from arrival in the NICU to start of UL placement. Plan-do-study-act (PDSA) cycles included: #1 Role clarification and work flow improvement for DR team. #2 Application of skin barrier for nasal NIV in DR prior to transport to NICU. #3 Development of a mobile stand outfitted with a t-piece resuscitator, oxygen blender, transport ventilator, intubation and NIV supply bags, and cylinder holders for air and oxygen tanks. #4 Education and simulation for DR team prior to roll out. #5 Implementation of mobile system and ongoing feedback collected to improve device performance.
Results:
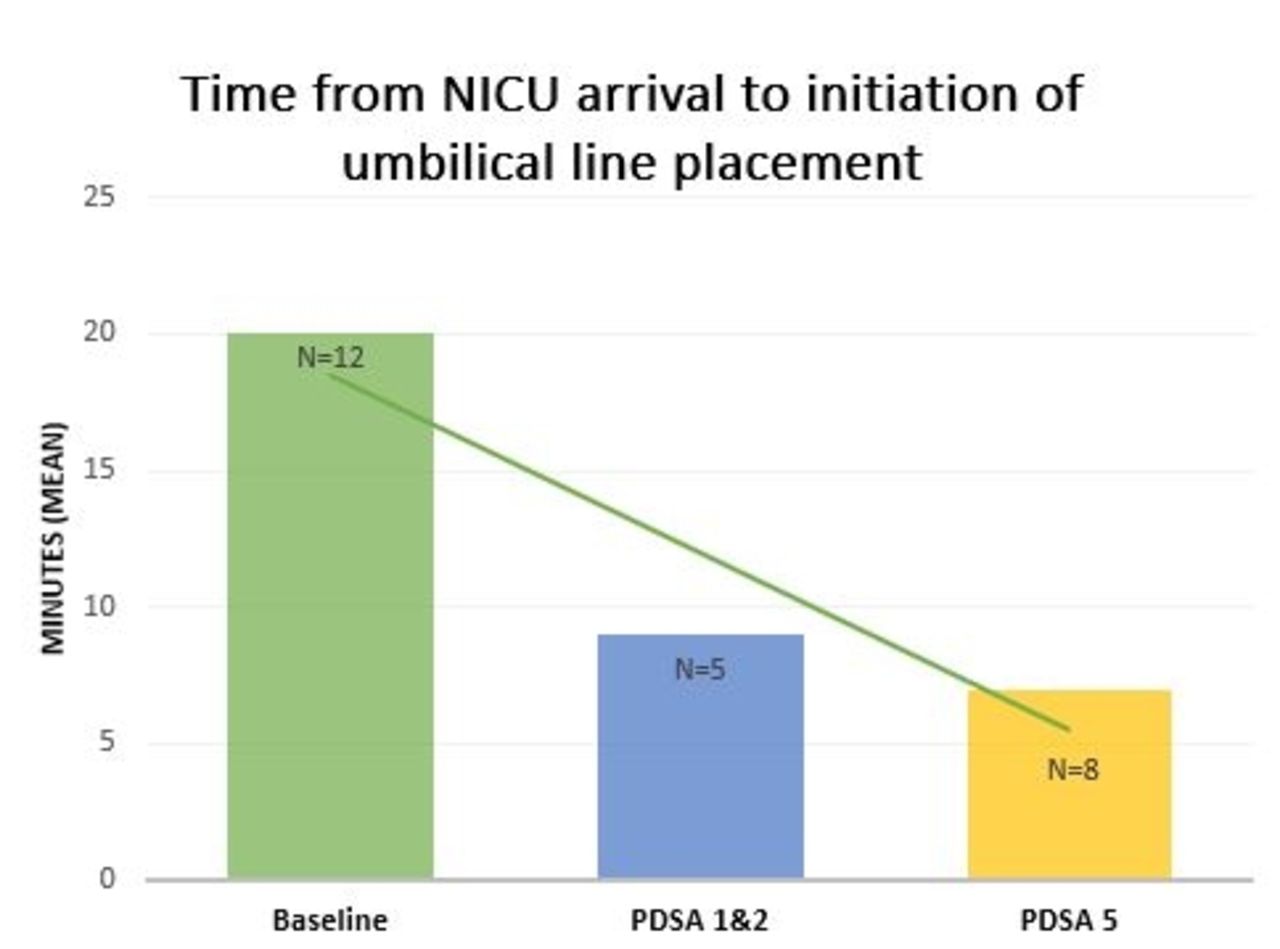
Base line data collected over 3 months showed the average time from NICU arrival to UL placement was 20 minutes (n = 12). After all PDSA cycles, this time decreased to 7 minutes (n = 13), a 65% reduction over a 5-month period. (Figure 1). As a balancing measure, data showed the average time from birth to NICU arrival was 24 minutes (baseline) and 23 minutes (post-intervention).
Conclusions:
Improvements in team workflow and implementation of a standalone mobile respiratory support unit demonstrated success in improving key time measurements in the first hour of life for preterm infants without increasing time spent in the delivery room or delaying arrival to the NICU.
Get full access to this article
View all access options for this article.