
Abstract
Background:
In the fall of 2016 as we aligned with Cleveland Clinic Alliance Network, it became clear that we had a significantly larger cardiac bypass and graft (CABG) patient population experiencing prolonged mechanical ventilation versus the national STS data. From January through September 2016, we had 11 patients (9.7%) receiving mechanical ventilation for >24 hours post-operatively versus the national Society of Thoracic Surgery database at 7.9%.
Methods:
Using the Plan-Do-Study-Act (PDSA) approach, an interdisciplinary team was formed comprised of RNs, providers, RTs, physical therapy and pharmacy. An early extubation protocol was developed to guide all disciplines within all phases of care from pre-operative to post-extubation. Once implemented, ongoing evaluation of patient outcomes and caregiver feedback supported a continued PDSA cycle.
Results:
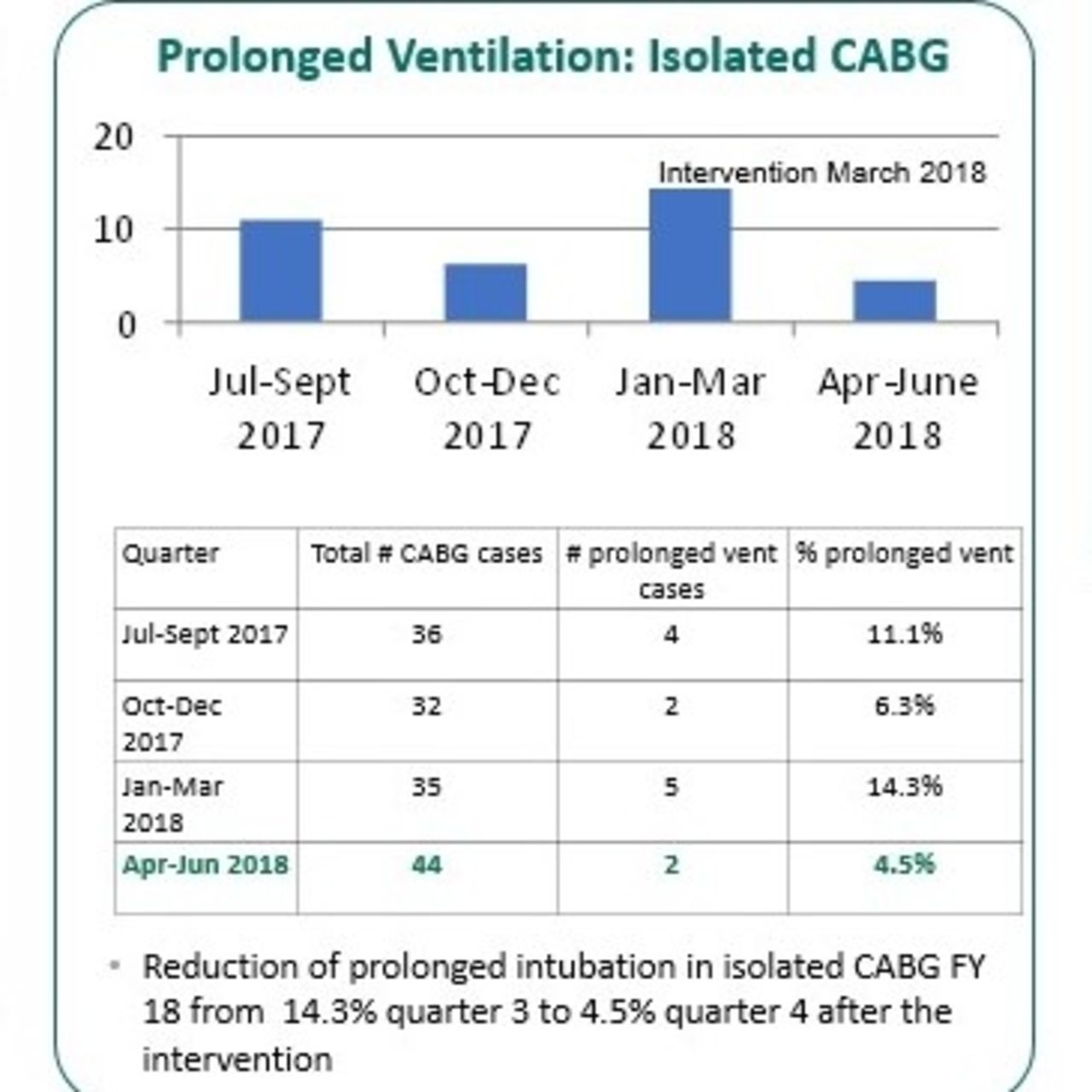
In fiscal year 2018 an increase of prolonged ventilation occurred. Interdisciplinary quarterly meetings were established to review cardiac surgery prolonged ventilation cases and determine trends. Challenges were also identified: three new cardiac surgeons joined our hospital in 2017, case volume increased by 21% (311 procedures in FY2017 to 376 in FY2018). We experienced an increase in high acuity cases such as ventricular assist devices (VADs), heart transplants, etc. that made up almost 33% of the total cardiac cases. After identifying the obstacles, changes were made utilizing the PDSA model. Changes made included new approach to identifying patient trends, broadened eligibility criteria and a 20-hour bedside huddle with RT, RN and provider if patient was still intubated. Once the protocol was established, the process saw impressive results regarding the percentage of CABG patients with prolonged ventilator times during our fiscal year 2017: Q1 8%, Q2 14.3%, Q3 (roll out of early extubation protocol) 3.7% and Q4 0%. In fiscal year 2018, a resurgence of prolonged mechanical ventilation after the success in fiscal year 2017: FY2018: Q1 11.1%, Q2 6.3%, Q3 14.3%. After the interdisciplinary workgroup made modifications using the PDSA model which led to a reduction of prolonged ventilation in Q4 to 4.5%.
Conclusions:
An interdisciplinary approach is necessary to facilitate and maintain the process of striving for early extubation in cardiac surgery patients. We incorporated this process for all cardiac surgery types in our CVICU and continue to meet as a team on a quarterly basis to review and adjust our protocol as needed utilizing the PDSA model.
Get full access to this article
View all access options for this article.