
Abstract
Background:
Rural hospitals have a difficult time recruiting pulmonologists and intensivists; not every provider in the Sarah Bush Lincoln Health System (SBLHS) has ventilator privileges. Historically, challenges have been receiving timely orders, evaluating vent settings, and aggressive weaning. Current research suggests RT driven protocols are safe and efficient ways to manage ventilated patients.
Methods:
An RT and RN driven protocol was co-developed and adopted to better facilitate a more consistent ventilator weaning process for patients. Beginning in January 2018, an algorithm was piloted at SBLHS. Patients were evaluated daily by nursing with a safety screen and subsequent spontaneous breathing trial (SBT) by RT if the patient qualified. During the vent weaning process, and upon completion of the SBT, patients are evaluated by a remote telemedicine multidisciplinary team comprised of RT, RN, and an intensivist. Upon successful completion of a SBT, even if a SBLHS provider is unavailable, a remote telemedicine intensivist can provide optimization or extubation orders. Examples of optimization orders may be changes such as sedation, vent settings, further blood gas analysis or a repeat wean trial later in the day. Continuous feedback and case reviews were evaluated along the way.
Results:
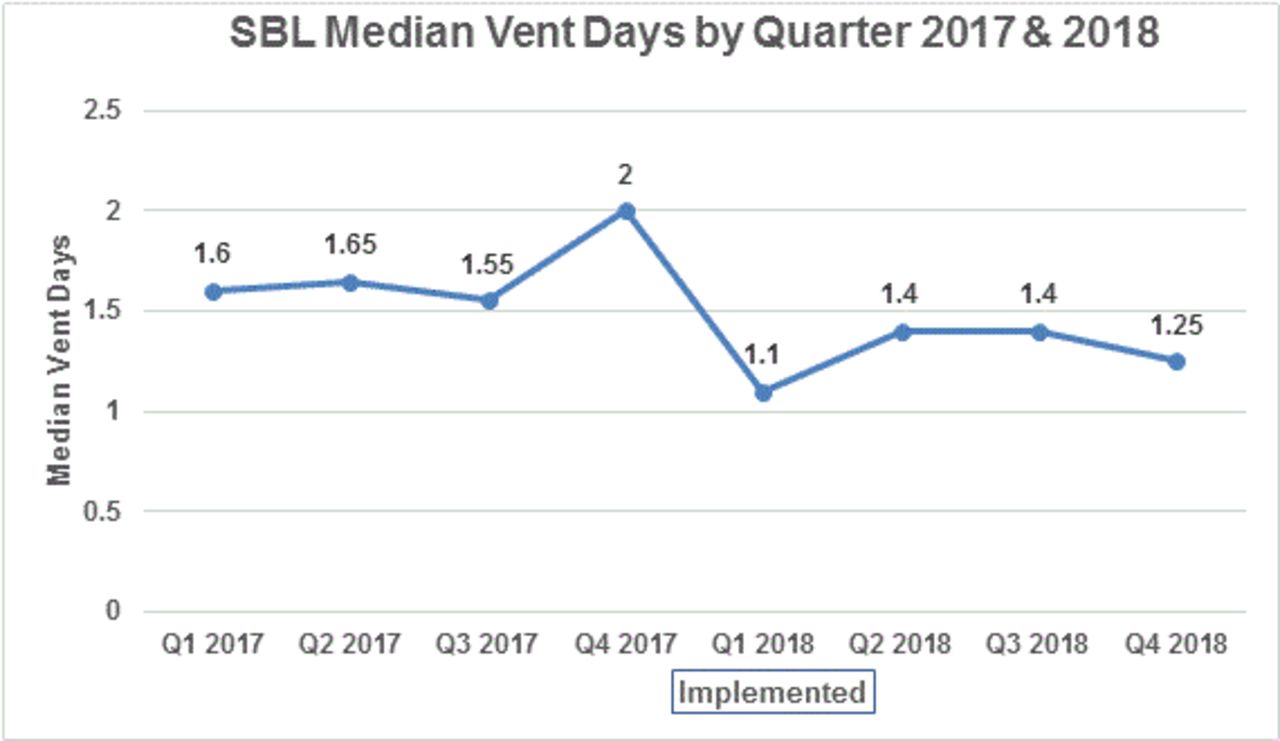
Two years of data was collected and evaluated. In 2017 and 2018, SBLHS had a total of 220 ventilated patients in our adult CCU. The top three diagnoses of patients who were maintained on ventilators were sepsis, surgery, and overdose, which account for nearly 63% of all intubated patients at SBLHS. One year after implementing the weaning process, our critical care unit saw a 24% reduction in median vent days.
Conclusions:
The addition of telemedicine support allows for timely provider orders and supports the bedside CCU staff with the vent weaning process. Regardless of time of day, this weaning process has improved communication and collaboration at the bedside through telemedicine support. This support has optimized ventilated patient outcomes, by decreasing ventilator days. RT and RN led protocols with the support of telemedicine have decreased median vent days in a rural community hospital. This study helps to set the stage for other opportunities that might exists between RT/RN led quality metrics. Barriers to this data include staff and provider buy-in. This study was approved by the institutional IRB. Disclosures: None
Get full access to this article
View all access options for this article.