
Abstract
Background:
Texas Children’s Hospital (TCH) is located in Houston, Texas. The TCH Newborn Center has 173 beds in three units. TCH Newborn Center manages approximately 25 intubated infants per day with 480 Registered Nurses (RNs), 130 physicians/Neonatal Nurse Practitioners (NNPs), and 50 Respiratory Therapists (RTs). Ues are the fourth most common cause of harm in Neonatal Intensive Care Units in the United States, with approximately 20% resulting in cardiovascular collapse requiring CPR or epinephrine.
Methods:
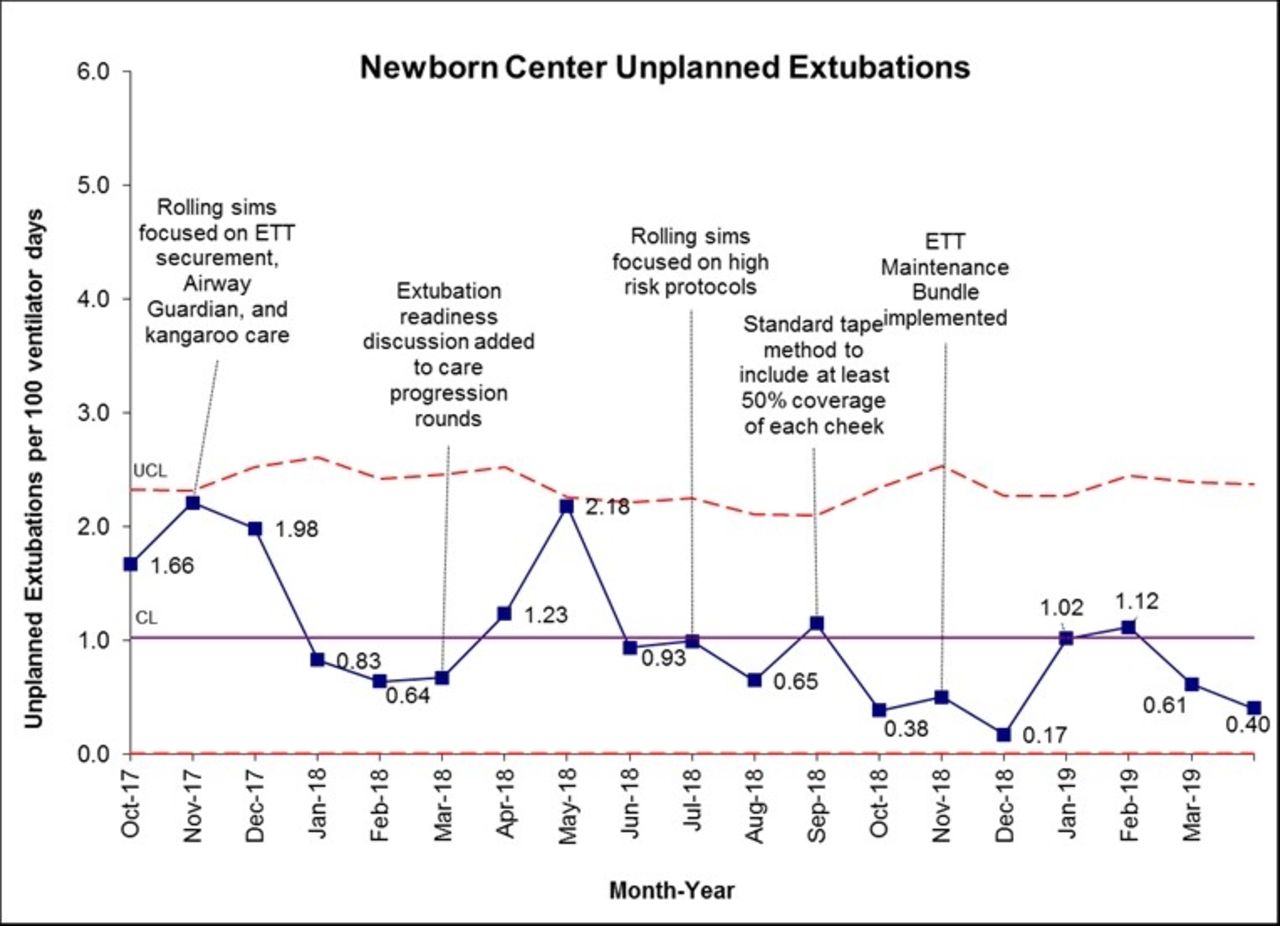
The Unplanned Extubation (UE) team is comprised of RNs, RTs, physicians, and NNPs that meet weekly to review any Ues from the preceding week and determine trends and potential interventions to help decrease the incidence. Each UE event has a debrief form completed, an in house safety event generated and is documented in the electronic medical record. In the weekly meetings all of the documentation is reviewed and events surrounding the UE are examined to determine a category in which to place the event. The primary categories are depth of the endotracheal tube (ETT), securement device failure, high risk activity (repositioning, weighing, bathing), agitation and unable to theme. The interventions developed and deployed to the units were, the WHERE Campaign, Weight Helps Ensure Right ETT depth, the NRP recommendation for ETT depth was used, weight in kg + 6 = approximate depth of the ETT at the lip. Utilization of an Airway Guardian to maintain the ETT during positioning, movement and invasive procedures. ETT securement was standardized to either tape or a commercial securement device. Rolling simulations were performed throughout the units on both shifts to facilitate comfort with standing transfers for Kangaroo Care. The last intervention looked at the standard ETT securement with tape and was more prescriptive over the amount of cheek coverage that should be attained, with a goal of at least 50% coverage of the area from the corner of the mouth to the ear.
Results:
The UE rate in the Newborn Center from October 2015 to September 2016 was at a high of 2.93 Ues per 100 ventilator days, this was reduced by 41% to a rate of 1.74 over the following year. The rate has continued to decline and in May 2019 has reached our lowest level with 0.4 Ues per 100 ventilator days.
Conclusions:
Despite the challenges of separate units and a large number of people to educate, a concerted and dedicated team can affect sustainable improvement and effect a culture change.
Get full access to this article
View all access options for this article.