
Abstract
Background:
There is increasing interest in administration of aerosol to patients requiring oxygen via high flow nasal cannula (HFNC). In vitro and radiolabeled in vivo studies concur that aerosol delivery decreases at higher flows (as low as 2.2% at 50 L/min) raising the question of what dose would achieve a clinically relevant bronchodilator response. Our objective was to administer doubling doses of albuterol to identify the maximum bronchodilator response in subjects who previously demonstrated response to bronchodilator in the PFT lab per ATS/ERS criteria.
Methods:
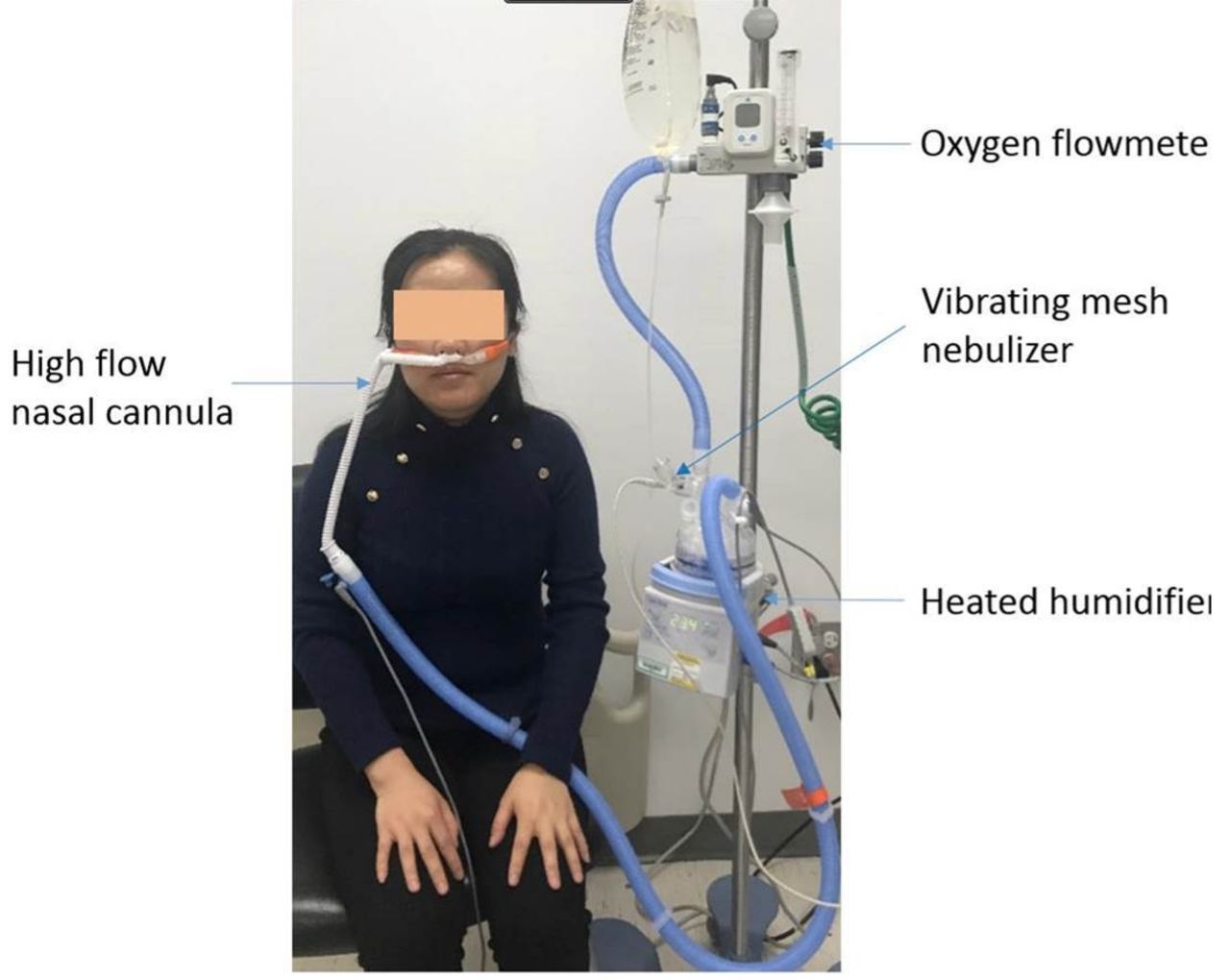
This study was approved by ethical committees at People's Hospital of Xinjiang, China and Rush University, Chicago and registered in clinicaltrial.gov (NCT03091504). Ambulatory subjects with obstructive lung disease who demonstrated bronchodilator response per ATS/ERS criteria were recruited to return after a washout period >24 hours to inhale doubling doses of albuterol delivered by mesh nebulizer (Aerogen Solo) via heated HFNC (Fisher & Paykel) at 50 L/min. Dose of 0.5, 1.0, 2.0, and 4.0 mg, diluted to 2 mL, was administered at 10-15mins interval. Spirometry was performed at baseline and after each dose. Dose escalation continued until FEV1 improvement was less than 5%.
Results:
42 subjects (15 male) with asthma (29) and COPD (13) were consented and completed study. Screening post bronchodilator FEV1 using MDI with valved holding chamber (VHC) at (mean ± SD) was 2.29 ± 0.72 L, After inhaling 0.5mg and 1.0mg of albuterol, FEV1 increased from 2.0 ± .66 L (baseline) to 2.23 ± .67 L (p < 0.01) and 2.34 ± . 7 L (p < 0.01), respectively, which was greater than post MDI+ VHC (P= 0.018). Eight subjects met termination criteria at 1.5mg. The remaining 34 subjects' FEV1 continued to increase slightly with cumulative 3.5mg dose, representing their max bronchodilator response (2.30 ± .68 vs 2.34 ± .69, p < 0.01). In a subset of COPD subjects, FEV1 stopped increasing at 3.5mg (1.99 ± .56 vs 2.04 ± .55, P=0.057). No serious adverse events were observed.
Conclusions:
Despite reported low inhaled dose efficiency (2.2%) with HFNC at 50 L/min, albuterol dose of 1.5 mg via HFNC produced improvements in FEV1 exceeding ATS/ERS definition of bronchodilator response in stable asthma and COPD patients. Maximal bronchodilator response occurred between doses of 1.5 and 3.5 mg.
Get full access to this article
View all access options for this article.