
Abstract
Background:
Pulmonary function tests rely on flow-volume loops (FVLs) to diagnose and monitor lung disorders and to assess reaction to broncho-constrictors or -dilators. The accepted standard for FVL generation is a spirometry-based forced vital capacity test, which requires patient cooperation. This often limits the utility of FVLs in pediatric patients or adults with limited ability to comply. For these patients, tidal breathing FVLs using respiratory inductance plethysmography bands were previously proposed but not widely adopted due to technology limitations. The objective of this study was to evaluate the utility of a non-invasive respiratory volume monitor (RVM) in measuring continuous tidal breathing FVLs in adult and pediatric patients in the perioperative period.
Methods:
After IRB approval, two clinical studies were conducted on adult and pediatric patients undergoing various surgical procedures under general anesthesia. A non-invasive RVM (ExSpiron1Xi, Respiratory Motion, Waltham, MA) was used to collect continuous respiratory volume traces intra- and post-operatively. Flow traces were generated by taking the first derivative of the volume traces. To reduce breath-to-breath variability, individual tidal breaths were aligned at the start of inhalation with volume and flow set to zero. Series of consecutive and similar breaths were grouped together. Individual breaths were divided into equal time segments and averaged across all breaths within a series to generate an average representative FVL for each patient during full mechanical ventilation, spontaneous breathing on the ventilator and spontaneous breathing post-extubation.
Results:
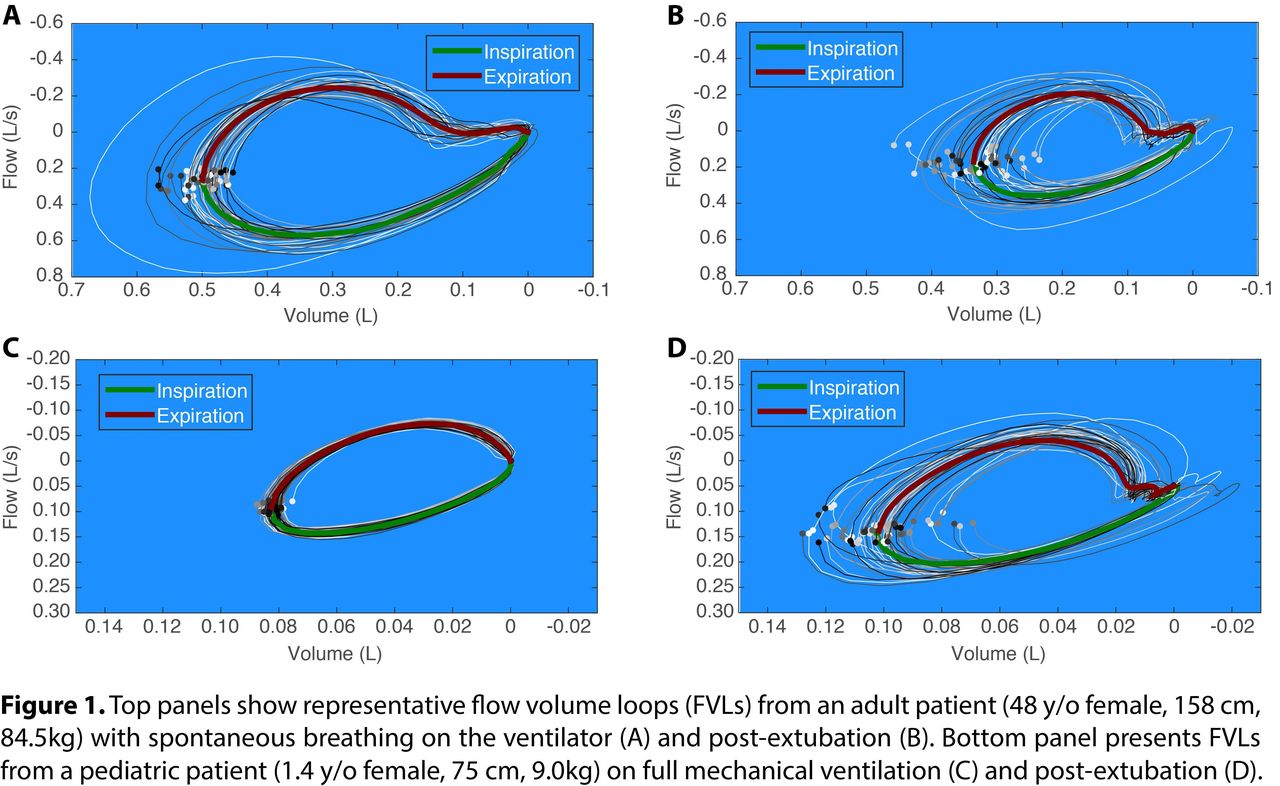
Preliminary data from 10 adult patients (5 males, age: 48. 3 ± 21.6 y; BMI: 29. 1 ± 6. 4 kg/m2, mean ± SD) and 10 pediatric patients (5 males, age: 5. 7 ± 4.9 y; BMI: 17. 3 ± 2.6 kg/m2, mean ± SD) were analyzed (Fig. 1).
Conclusions:
We demonstrate that the RVM can generate continuous tidal breathing FVLs in adults and children with distinct shapes based on breathing and mechanical ventilation. The RVM FVLs can theoretically be obtained for patients with pulmonary disease and potentially identify distinct breathing patterns related to disease diagnosis, progression, and response to therapy. The RVM may eliminate the need for bedside spirometry and vastly expand the applications of FVL analysis, especially in pediatric and non-compliant patients.
Disclosures:
None.
Get full access to this article
View all access options for this article.