
Abstract
Background:
An efficient method for delivering O2 via nasal cannula is needed in patients with chronic respiratory insufficiency. Liquid and compressed gas cylinders have several limitations, including: 1) portability; 2) cost; 3) ability to provide sufficient O2 duration outside of the domicile setting; and 4) space and safety considerations. Manufacturers now offer an array of commercially available portable oxygen concentrators (POCs) that provide a patient-triggered bolus of O2 to the nasopharynx. The objective of this bench study was to evaluate triggering and FDO2 with POC systems. We hypothesized that there would be no differences in FDO2 in spontaneously breathing lung models between standard O2 cannula and POC at different settings.
Methods:
Neonatal, toddler, small child, and adult 3D printed upper airway models were affixed to the Ingmar ASL 5000 via a series of one-way valves. A standard O2 cannula, seven POC systems and one oxygen-conserving device (OCD) were applied to the airway models using a range of settings. FDO2 measurements (n=20) were acquired from within the lung model following a brief stabilization period. We recorded triggering based on a digital indicator on the POC that coincided with lung model inhalation.
Results:
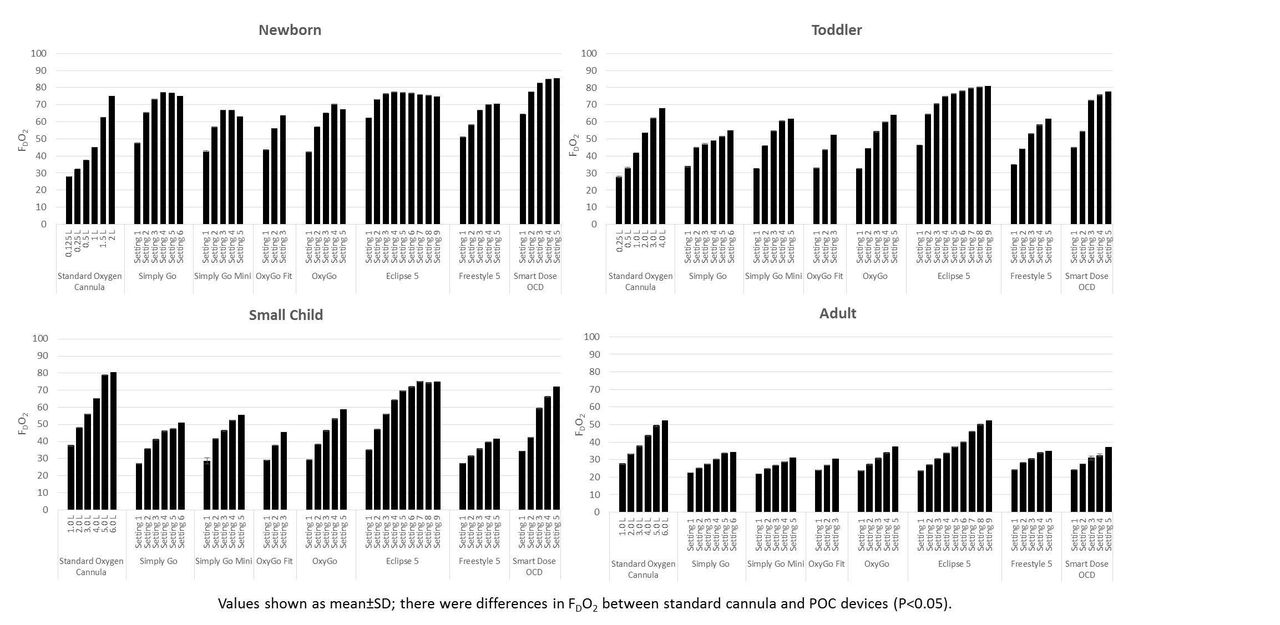
POC devices allowed consistent triggering of O2 boluses across all of the testing conditions and models, except for one, which triggered boluses every other breath in the term newborn model. This manufacturer chose not to include this device in our post-analysis report. FDO2 measurements between standard O2 cannula and POC devices was different (see figure, P<0.05) and dependent upon the specific lung model and POC bolus size. FDO2 was consistently greater with some POC devices than O2 cannula (P<0.05) in the newborn model.
Conclusions:
The major finding from this study is that all simulated patient models were able to trigger all POC devices. Special consideration for use of POCs in the newborn must be given as bolus sizes are not specifically tailored to be used in patients with smaller airways and tidal volumes. Care must be taken in selecting POCs and titrating doses based on individual patient oxygenation needs. Future studies are needed in order to determine whether POC devices are able to support patients with different lung diseases.
Get full access to this article
View all access options for this article.