
Abstract
Background:
Unplanned Extubation (UE) in pediatric patients can increase length of stay by 6.5 d/case and cost on average $36,692/case. Risk factors, such as age, gender, increased oral secretions, intubation duration, nursing ratios, ETT fixation method and sedation have all been referenced in the literature. Harm caused by UE can be catastrophic and sometimes result in death. Re-intubation after UE can also cause a higher incidence of ventilator-associated pneumonia (VAP) and a 3-21% higher mortality rate. In an effort to reduce VAP and the potential of harm caused by UE in the PICU, we began to monitor our UE rate and compared our performance with comparable pediatric facilities. After observing that our UE rate was higher than the national average of 0.74 per 100 ventilator days, we decided to implement clinical standardization to minimize the risk. During our investigation, it was noted that most of our UE events were possibly related to the securement device. We focused on efforts on standardizing a process for tube securement, based on the ETT size.
Methods:
Phase 1 included an IRB approved retrospective data analysis from 7/1/2016 to 6/30/2017 of UEs per 100 vent days. Phase 2 included implementing a standard ETT securement method within the pediatric intensive care unit (PICU). Education for respiratory therapists and nurses on the securement devices was performed formally. For all patients with ETTs < 4.0 mm a CooperSurgical NEO-Fit securement device was utilized, and for ETTs > 5.0 mm, a Hollister Anchorfast securement device was utilized. ETTs = 4.5mm were taped using our previous standard taping method due to lack of securement devices available on the market approved for use with that size. Phase 3 included prospective data collection from 7/1/2017 to 5/30/2018 of UEs per 100 vent days.
Results:
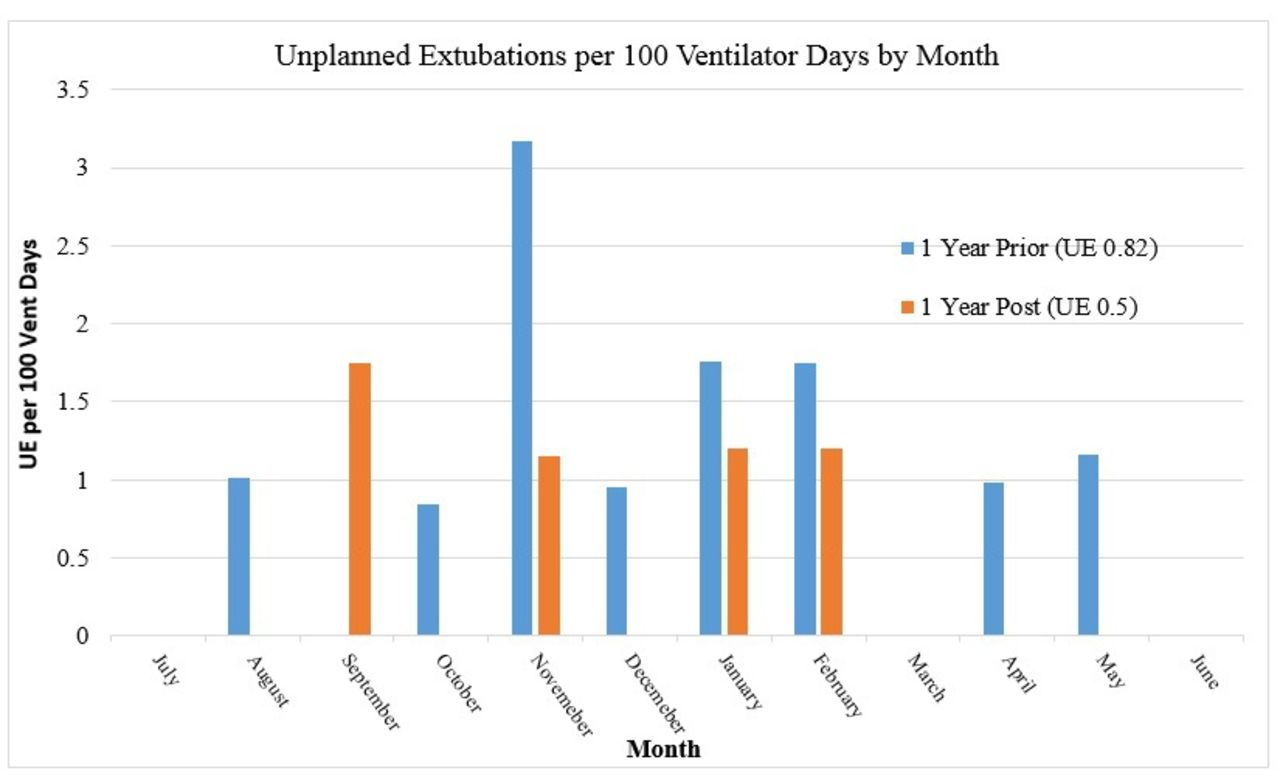
The UE rate from 7/1/2016 to 6/30/17 of UEs was 0.82 per 100 ventilator days (11/1327). After initiation of a standardized securement device usage, the UE from 7/1/17-5/30/18 decreased to 0.50 per 100 ventilator days (5/992). The total number of UEs in year one was 11, compared to 5 UEs in year two, post standardization securement.
Results:
See graph for detailed month-to-month data.
Conclusions:
In conclusion, the rate of UE decreased from 0.82 to 0.50 incidences per 100 ventilator days in an approximate 2-year period. Based on these data, the implementation of a standard process for ETT securement has a positive impact on UE rate.
Get full access to this article
View all access options for this article.