
Abstract
Background:
Inhaled Nitric Oxide (INO) is an effective pulmonary vasodilator used in intubated children with hypoxic respiratory failure. Recent evidence supports the use of early noninvasive ventilation (NIV) following extubation from mechanical ventilation. In many cases, patients will remain intubated because it is unknown whether INO can be delivered safely/effectively with NIV, especially when a single-limb BPAP circuit is used. We hypothesized that there would be no differences in INO/NO2 delivery, PEEP, and volume in a spontaneously breathing toddler lung model between different INO/NIV device configurations.
Methods:
A 3D printed toddler airway model was affixed to an ASL 5000 test lung (IngMar Medical). A KMNO4/charcoal filter was placed proximal to the lung model to eliminate re-breathing of exhaled INO/NO2. The INOmax DSir (Mallinckrodt Medical) was used to administer INO at 20 and 40 ppm with the following NIV delivery options: 1) Trilogy 202/single limb circuit with vented nasal and oronasal masks. 2) Trilogy 202/single limb circuit oronasal mask with INO delivered via HFNC 2-12 L/min. 3) Draeger ventilator/dual-limb circuit with non-vented nasal and oronasal masks. Tracheal NO and NO2 levels were measured between the 3D model and test lung with INOmax DSir electrochemical sensors. Pressures and volumes were obtained from within the test lung. Accuracy of INO was determined by calculating % error= (tracheal NO-preset INO level) /preset INO level*100. Differences in INO, PEEP, and VT between the delivery options were compared using ANOVA.
Results:
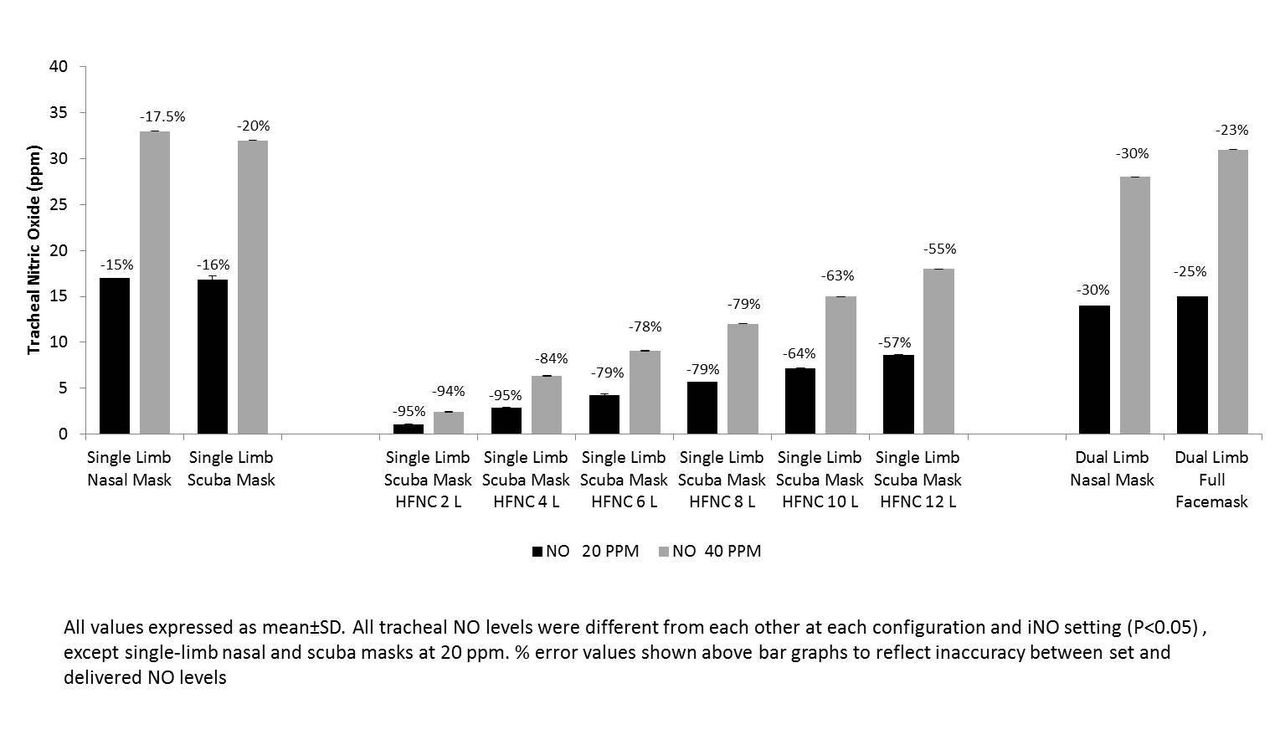
All NO2 levels were <1 ppm. PEEP levels (>1 cm H2O above the set PEEP value) occurred more frequently with HFNC/single-limb Trilogy than other configurations (P<0.05). Sampling/adding INO did not appear to have any effect on delivered volumes. INO therapy delivered with single-limb circuit provided greater NO levels (P<0.05) and with greater accuracy (P<0.05) than the other INO/noninvasive delivery configurations (see Figure).
Conclusions:
Based on our findings, it appears INO delivery may be delivered more effectively using a single-circuit/vented-mask than other INO/noninvasive configurations. Providing INO through HFNC/mask appears to have a flow-dependent increase in PEEP with very little INO delivery to the lung model. Future studies are suggested, using > 30 kg models to determine whether these INO delivery options are safe/effective in adult-sized patients.
Get full access to this article
View all access options for this article.