
Abstract
Background:
Minimizing mechanical ventilation (MV) days reduces the risk of VAP, morbidity and mortality. Extubation readiness is traditionally based on subjective information; extubation failure is not. A review of the literature reveals that extubation failure occurs due to: apnea, poor cough/gag, escalating support, Oxygen Index>6 on non-cyanotic heart, PEEP>5 on cyanotic heart, frequent suctioning, CO2 retention, or FIO2 50%. We sought to compare outcomes of an extubation readiness assessment (ERA) protocol with directed weaning by respiratory therapists (RTs) and traditional physician-directed (PD) weaning from MV on ventilator days, MV >21 days, unplanned extubations (UE), and ventilator-associated pneumonia (VAP) in pediatric cardiovascular care unit (CVICU) subjects.
Methods:
An IRB approved prospective observational cohort design study was conducted on all intubated CVICU subjects from 11/01/16 - 10/31/17 who met objective inclusion criteria. Subjects were assigned to ERA or PD based on physician preference. ERA subjects were assessed daily for eligibility, and if eligible were placed on CPAP/PS. ERA failure was defined as not consistently maintaining respiratory and cardiovascular goals. Subjects on MV<12 h were factored out of MV time because they were not on MV long enough to be assigned to ERA or PD group.
Results:
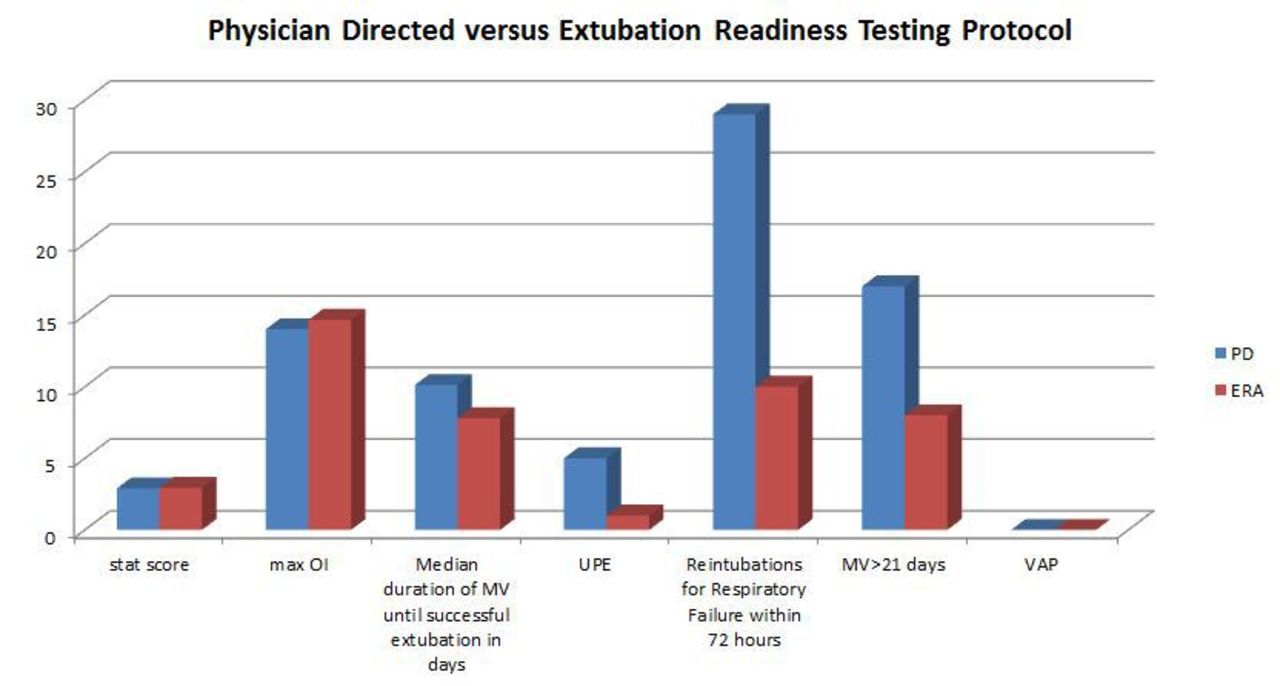
Of 481 intubation events, 122 were enrolled in ERA (median STAT score 2.94 and max OI 14.66). 122 (100%) were extubated within 0-23 (mean 6.03) h of passing the ERA, including 112 (91.80%) who were extubated for more than 72 h. Time on MV until successful extubation ranged from 0.04-63.83 d. The median duration of MV was 7.8 d for subjects on MV > 12 h.8 subjects had MV >21 d. One UE occurred that did not require re-intubation. Of 483 intubation events, 359 were enrolled in PD weaning (median STAT score= 2.90 and max OI= 14.01). Of these 330 (91.90%) were extubated for more than 72 h. Time on MV until successful extubation ranged from 0.01-103 d. The median duration of MV was 10.12 in subjects on MV >12 h. 17 subjects required MV >21 d.5 had UE (1.4%), with 3 requiring re-intubation.
Conclusions:
ERA protocol performed by respiratory therapists to assess extubation readiness in pediatric CVICU led to less median duration of subjects on MV >12 h, less subjects on MV >21 d (P=0.089), and less UE than PD weaning (0.621), but did not reach statistical significance.
Disclosures:
None.
Get full access to this article
View all access options for this article.