
Abstract
Background:
Meeting patient care needs and labor budget should be synonymous in nature. In fact, many respiratory care departments struggle with aligning these two necessary metrics. The AARC created the Uniform Reporting Manual (URM), an evidence-based benchmark to reflect the productivity of therapist time spent at the bedside performing care. Yet, many hospitals do not incorporate these standards to create labor budgets. This study analyzed the use of a hybrid assignment tool to bridge the gap between therapist workload reality and a commercially available labor management/budget program.
Methods:
A thorough analysis was conducted comparing and matching the 2012 URM to the procedural charge master for Levine Children's Hospital. All procedures were broken into 15-min increments for ease of use and assigned based on the time standard provided by the URM. Example: SVN is assigned 15 min = 1 point, a ventilator is assigned 60 min = 4 points. This accounts for the acuity of each patient as they are different. Respiratory therapists work 12 h, which equates to 10.5 h of value-added bedside care. This means that every therapist can perform 42 points worth of work safely. Our established target assignment is 36 points to allow for a 10-15% "pick up" of unaccounted work. The assignment tool, created in Excel, was posted to our SharePoint site for ease of use. Training was completed to ensure standard work. The effectiveness of the assignment tool was measured from 7/1/17 to 5/28/18 and compared to the daily Premier productivity report.
Results:
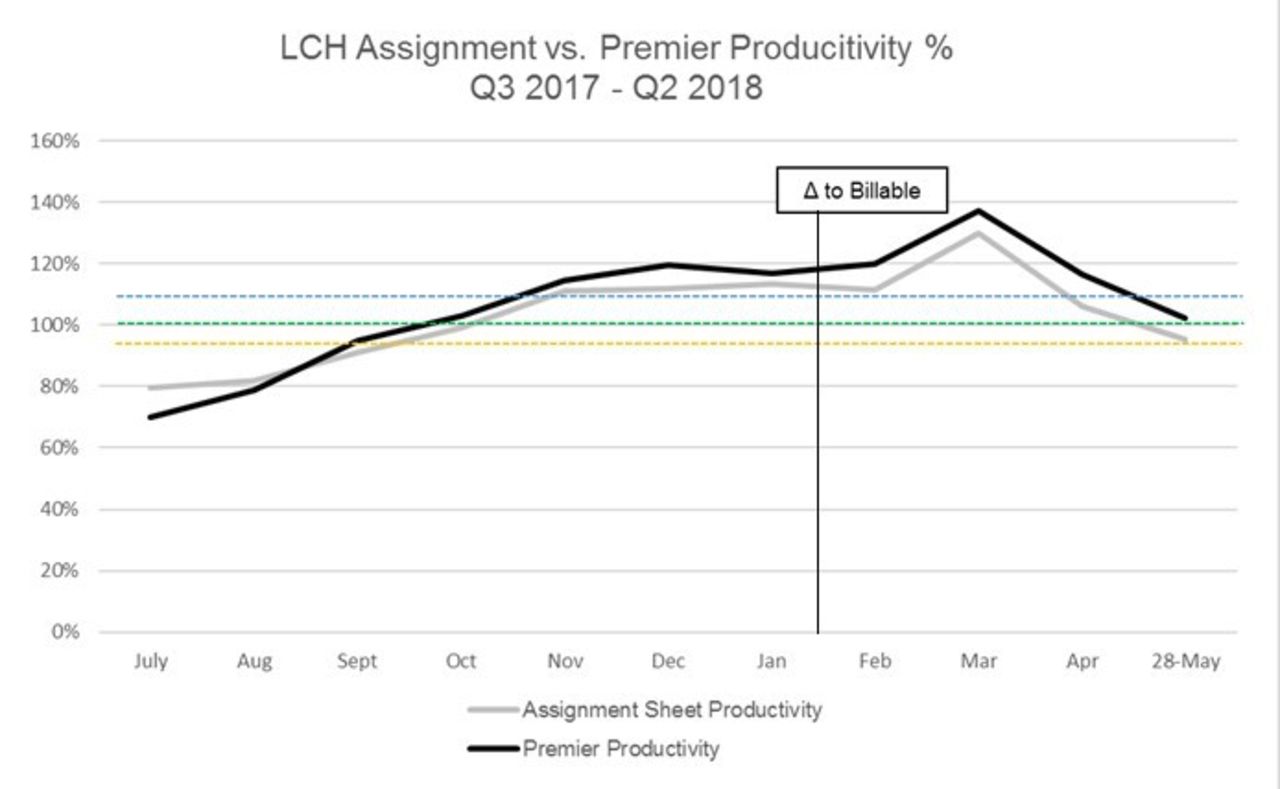
Comparison of the assignment tool and the daily productivity report yielded only a 3.9% difference (Assignment tool 102.77% YTD, Premier 106.67% YTD). Also, no change was noticed in January when our standard comparison group changed from all procedure count to billable only procedure count. The assignment tool also identified, in real time, the need/opportunity to flex staff to volume. This resulted in an estimated cost savings of $57,249.92 (or roughly 1 FTE). The tool is easily adaptable to meet future budgetary and acuity demands.
Conclusions:
Bridging the gap between commercially available labor management tools and workload reality is not impossible, it is simply an exercise in translation. Development, creation, and validation of a live, working assignment tool is an opportunity to bridge that gap to ensure optimal patient care while meeting budget.
Get full access to this article
View all access options for this article.