
Abstract
Background:
A dearth of research exists examining NIV use in a general population of sepsis patients (pts) with acute respiratory failure (ARF). NIV studies in ARF have included heterogeneous samples with some sepsis subjects but this group has not been the main focus. This study sought to review the clinical course and failure rates of pts with a diagnosis of sepsis and ARF placed on NIV.
Methods:
A retrospective analysis (IRB 2018-142) was conducted on all pts with a diagnosis of sepsis placed on NIV from July 2017-Mar 2018 using information from the EMR and other data repositories. Demographic and clinical outcome data were collected and analyzed using the chi-square test for categorical information, and Student t or Wilcoxon rank-sum tests for quantitative data, depending on normality results using Shapiro-Wilk. Uni- and multivariate logistic regression were conducted to determine predictive factors for NIV failure.
Results:
165 pts were reviewed with 52 excluded (OSA, extubated to NIV, palliative), leaving 113 ARF subjects with 59 in the NIV Fail group (NIVF; required intubation) and 54 in NIV Success (NIVS; no intubation). There were no statistically significant differences between groups for age (P=. 22), sex (P=.90), Charleson CI (P=. 26), immunosuppression (P=.94), sepsis source (pulmonary, extrapulmonary, mixed; P=. 20), PaCO2 (P=. 75) HCO3 (P=.65) or pH (P=. 18) within the 1st 2 h post NIV, lactate or HR prior to NIV (P=. 11 and P=.66, respectively), or acute on chronic RF (P=. 49). However, the NIVF group had a significantly lower median P/F ratio within the 1st 2 h post NIV (186.7 [106.7-210.6] v 227.5 [168.2-347.1]; P=.02) and mean arterial pressure (MAP) at NIV start (78 [68-93] v 92 [83-108] mm Hg; P<.001). In the NIVF group, RR (32 [23-38] v 22 [20-27] breaths/min; P<.001) and WOB (P<.001) were significantly higher within the 1st 2 h post NIV and more subjects in this group had an altered mental status (AMS; 59% v 28%, P=.001), shock (P<.001), ARDS (20% v 0, P<.001) and died (P<.001) compared to NIVS. From univariate logistic regression - source, shock, AMS, MAP, lactate, age and WOB were entered into a multivariate regression model. Source (P=.036), WOB (AUC .84 [CI . 78-.91]; P<.001), MAP (AUC 0.70 [CI 0.60-0.80] P=.001) and AMS (AUC 0.65 [CI 0.56-0.74) ; P=.001) were independently associated with NIV failure.
Conclusions:
MAP, AMS and WOB provided fair to good models, respectively for predicting NIV failure in subjects with sepsis and ARF. There were high NIV failure rates in these subjects.
Altered mental status (AMS), mean arterial pressure (MAP), sepsis source (intrapulmonary, extrapulmonary, and mixed; source), and work of breathing (WOB) were all independently associated with NIV failure in subjects with sepsis. MAP and WOB provided models with the best predictive values.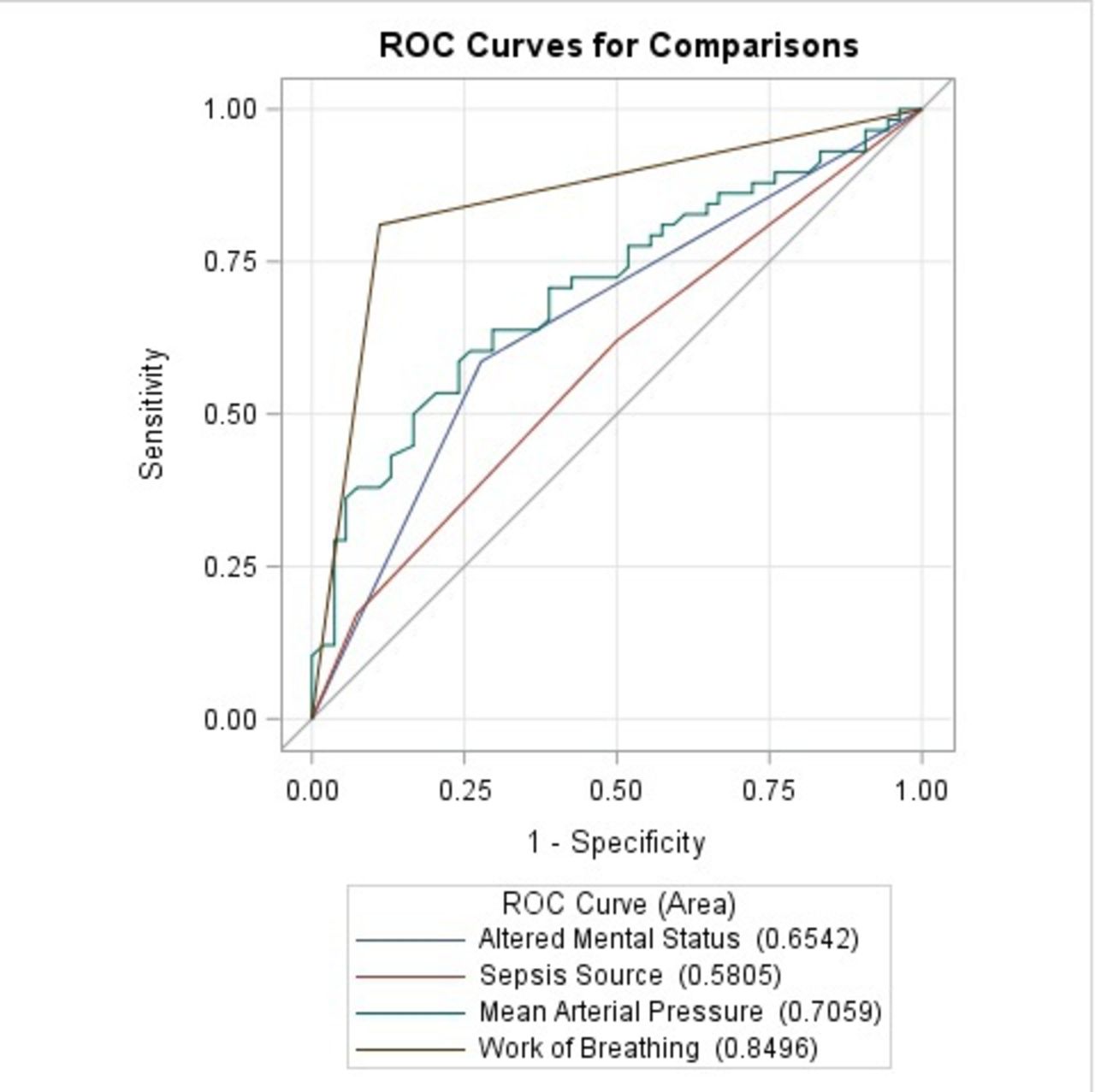
Get full access to this article
View all access options for this article.