
Abstract
Background:
Premature lungs are at a high risk of injury from mechanical ventilation. Pressure controlled ventilation, where respiratory therapists monitor and titrate peak inspiratory pressure to keep tidal volume within 4-7 mL/kg, is widely used in the neonatal intensive care unit. However, pressure controlled ventilation may expose the lung to volutrauma with changes in lung compliance and hypo or hyperventilation can increase the risk of injury to the premature brain. We sought to identify the variability of tidal volume during pressure-controlled ventilation in mechanically ventilated premature neonates.
Methods:
Data files of neonates < 32 weeks gestational age enrolled in clinical trials at the Neonatal Research Institute at Sharp Mary Birch Hospital for Women and Newborns were searched to identify infants who received pressure controlled mechanical ventilation in the first 72 hours of life. Mother and infant demographics and ventilator downloads were prospectively collected. Infants with major congenital anomalies were excluded from the primary studies. The ventilator internal clocks were set and routinely checked to synchronize with the electronic medical record. The exhaled tidal volume of a mechanical breath every 5 min was converted to mL/kg using birth weight. Parents of the infants gave consent for the primary trial. The Sharp Institutional Review Board approved the primary trials and the secondary data analysis.
Results:
Sixty-nine infants with ventilator data within the first 72 h of life were included. The mean gestational age was 27 ± 2 weeks with birthweight of 1,069 ± 378 g. A total of 1,533 hours of data or 18,397 breaths were analyzed and 11.9% of breaths were < 4 mL/kg, 31.6% were > 7 mL/kg, 10% > 9 mL/kg, and just 56.5% fell within the targeted 4-7 mL/kg (Figure 1).
Conclusions:
In this cohort 43.5% of the pressure control breaths were outside of the targeted volume range of 4-7 mL/kg.
Disclosures:
None.
Figure 1 Distribution of Tidal Volume During Pressure Control Ventilation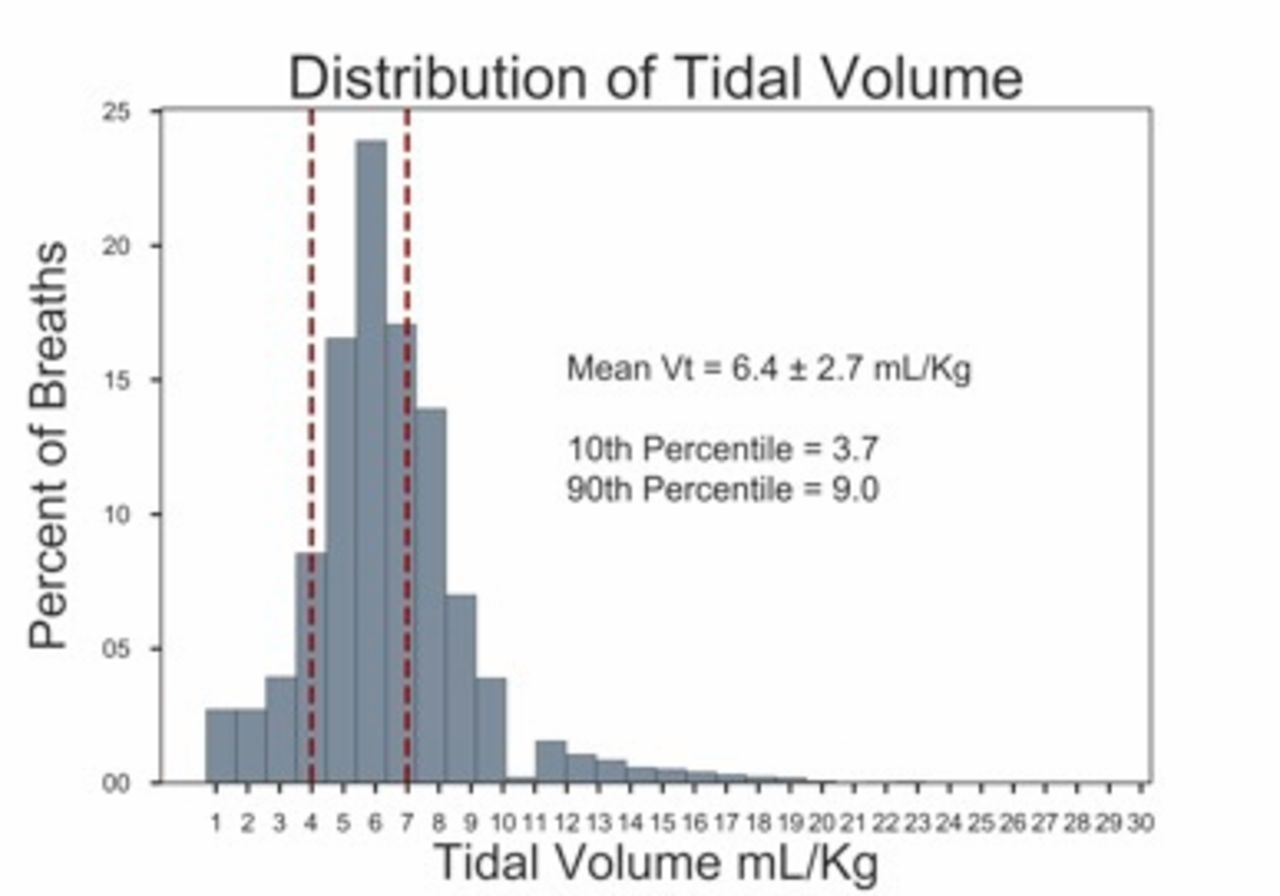
Get full access to this article
View all access options for this article.