
Abstract
Background:
For mechanical ventilation (MV) to reduce patient work of breathing (WOB) and respiratory muscle tension-time, or pressure-time product (PTP), requires the ventilator to displace the chest faster than inspiratory muscular contraction. This 'push-pull' concept first proposed by Marini et al,1 has great explanatory power in interpreting WOB study results. Modeling this interaction requires that simulated effort can potentially be overtaken by MV driving pressure (eg, proportional assist ventilation or PAV, pressure support ventilation or PSV). 2 We evaluated the impact of PAV+ and PSV on WOB using the IngmarASL-5000 (Pittsburg, PA) using a fixed breathing pattern at varying levels of simulated inspiratory muscle pressure (ΔPmus) .
Methods:
The ASL-5000 was set to a compliance of 35 mL/cm H2O, resistance of 5 cm H2O per L/s and was connected to PB-980 ventilator (Medtronic, Minneapolis, MN) using a 7.5 mm ID endotracheal tube. The ventilator was set to 3 levels of PAV+ (70%, 50%, 30%) and 4 levels of PSV (ΔP: 15, 10, 5 and 0 cm H2O). End-expiratory pressure of 5 cm H2O and trigger sensitivity of 3 L/min were used for all conditions. The breathing pattern was f of 20 breaths/min with ΔPmus of 5, 10 and 15 cm H2O; pressure rise, sustain and decay of 20%, 10%, 10% respectively (inspiratory time: 1.2 s). Multiple linear regression was used to assess variables determining simulated WOB. Alpha was set at 0.05.
Results:
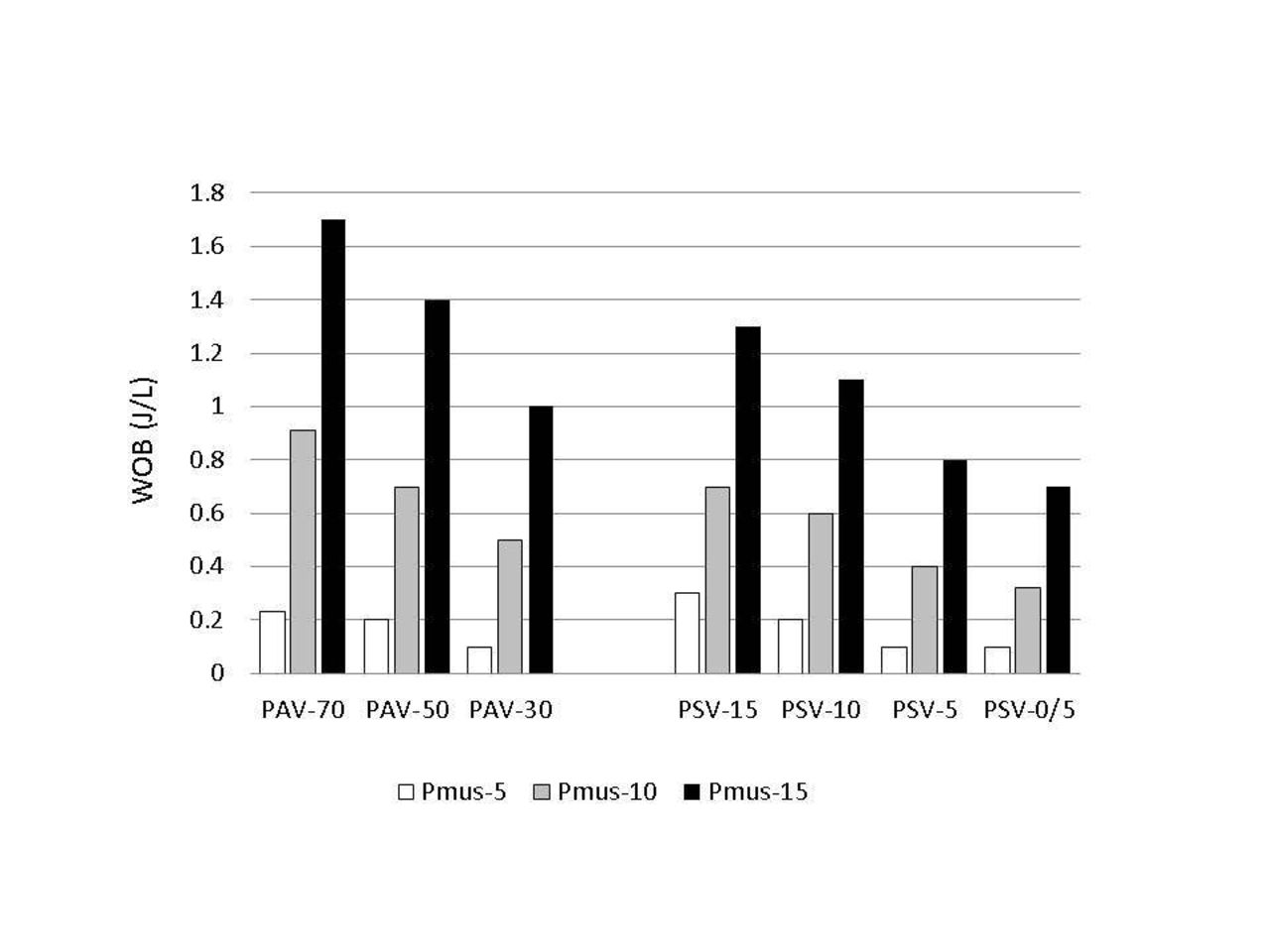
At all PAV+ and PSV settings simulated WOB paradoxically decreased with decreasing MV support (Fig). Simulated PTP was unaffected by MV support level on either mode at ΔPmus levels of 5, 10 and 15 cm H2O (110-112, 220-224 and 334-336 cm H2O-s per min respectively). WOB was positively correlated with VT (t-ratio: 4.82, P < 0.001) but not with PTP/b (t-ratio: 0.29, P= 0.77) as a signifier of simulated effort. VT was more strongly correlated with peak inspiratory pressure (t ratio: 10.4, P < 0.001) than with PTP/b (t-ratio: 6. 3, P<0.001)
Conclusions:
WOB is defined as the area within the Pmus-VT loop. As such when VT decreases at a constant Pmus so too does WOB. A model wherein Pmus cannot be replaced by positive pressure cannot reflect what occurs under in vivo conditions.
1. Marini JJ, et al. The inspiratory workload of patient-initiated mechanical ventilation. Am Rev Respir Dis 1986;134:902-909. 2. Katz JA, et al. Inspiratory work and airway pressure with continuous positive airway pressure delivery systems. Chest 1985;88:519-526.
Get full access to this article
View all access options for this article.