
Abstract
Background:
The air entrainment Venturi mask (VM) is a widely used oxygen administration device. Along with VM, the manufacture (Everestmed-equip, Taiwan) also provides collars, which can be combined with large volume nebulizers (VMLVN) to decrease nose and mouth dryness. However, the cold and moist mist can cause the side effects of bronchoconstriction. Previous studies were all unable to provide a standard method for using VM combined with a heated humidifier (VH-1500, Taiwan); (VMH). Therefore, this study aimed to analyze and compare changes in the oxygen concentration and total flow between VMH and VMLVN using an oxygen analyzer and examine the feasibility of VMH.
Methods:
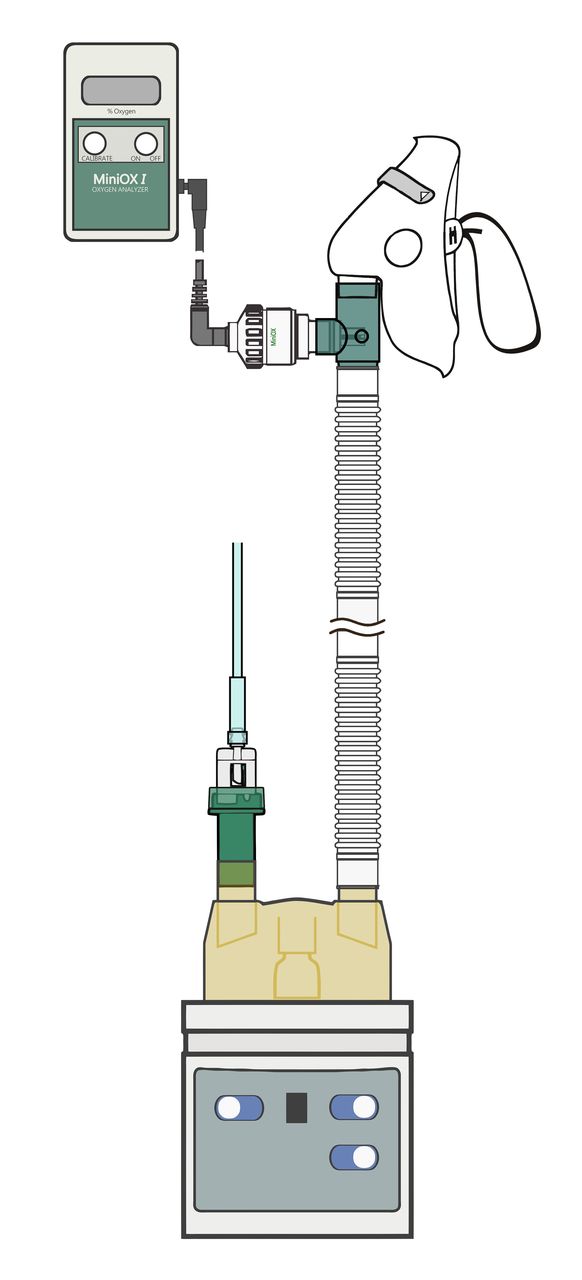
This study uses VMs manufactured in Taiwan. Twenty-one samples were randomized into two groups, namely VMH and WMLVN. Under seven FIO2 concentrations and flow conditions (24% 3 L/min, 26% 3 L/min, 28% 6 L/min, 30% 6 L/min, 35% 9 L/min, 40% 12 L/min, and 50% 15 L/min), an oxygen analyzer was used to repeatedly monitor changes in the FIO2 concentrations in the first 1, 5, and 10 min and the mean values were calculated. The total flow formula (79 x O2 flow) / (O2% – 21) was used to obtain the total flow. Repeated measurements were used to identify dependence, and the Mann—Whitney U test was used to compare differences between the two groups.
Results:
The Table shows the seven oxygen concentrations and total flows measured in the VMH and VMLVN groups. Results showed no significant differences in the FIO2 concentrations measured in the first 1, 5, and 10 min between the groups (P > 0.05). The mean and standard deviations of the VMH and VMLVN groups were 41.0% ± 2.0% and 29.2 ± 1.7 L/min and 33.5% ± 1.9% and 54.2 ± 2.3 L/min, respectively. The FIO2 concentration of VMH was significantly higher than that of VMLVN (P < 0.05), whereas the total flow of VMLVN was significantly lower than that of VMH (P<0.05).
Conclusions:
Our study found that the oxygen concentration of VMH was higher than that of VMLVN, whereas the total flow of VMH was lower than that of VMLVN, which suggests that an increase in the oxygen flow decreases air entry and, thereby, affects the total flow. Therefore, in clinical practice, a patient's flow demand may not be fulfilled, which affects the patient's inhaled oxygen concentration. Therefore, we recommend that patients' respiration pattern and inhaled oxygen flow should be re-evaluated when using VMH to fulfill their flow demand.
Get full access to this article
View all access options for this article.