
Abstract
Background:
Recently there has been some discussion on using 2.0 endotracheal tubes (ETTs) in the neonatal patient population. Recent advances in technology and the medical community has expanded resuscitation to smaller patients that require smaller ETTs. Very little data exist on performance of 2.0 ETTs in conjunction with the high frequency jet ventilator (HFJV). We developed a bench testing strategy to evaluate the 2.0 ET tube and Bunnell LifePulse 204 (HFJV) ventilator (Salt Lake City, Utah) in our test lung (TL) model.
Methods:
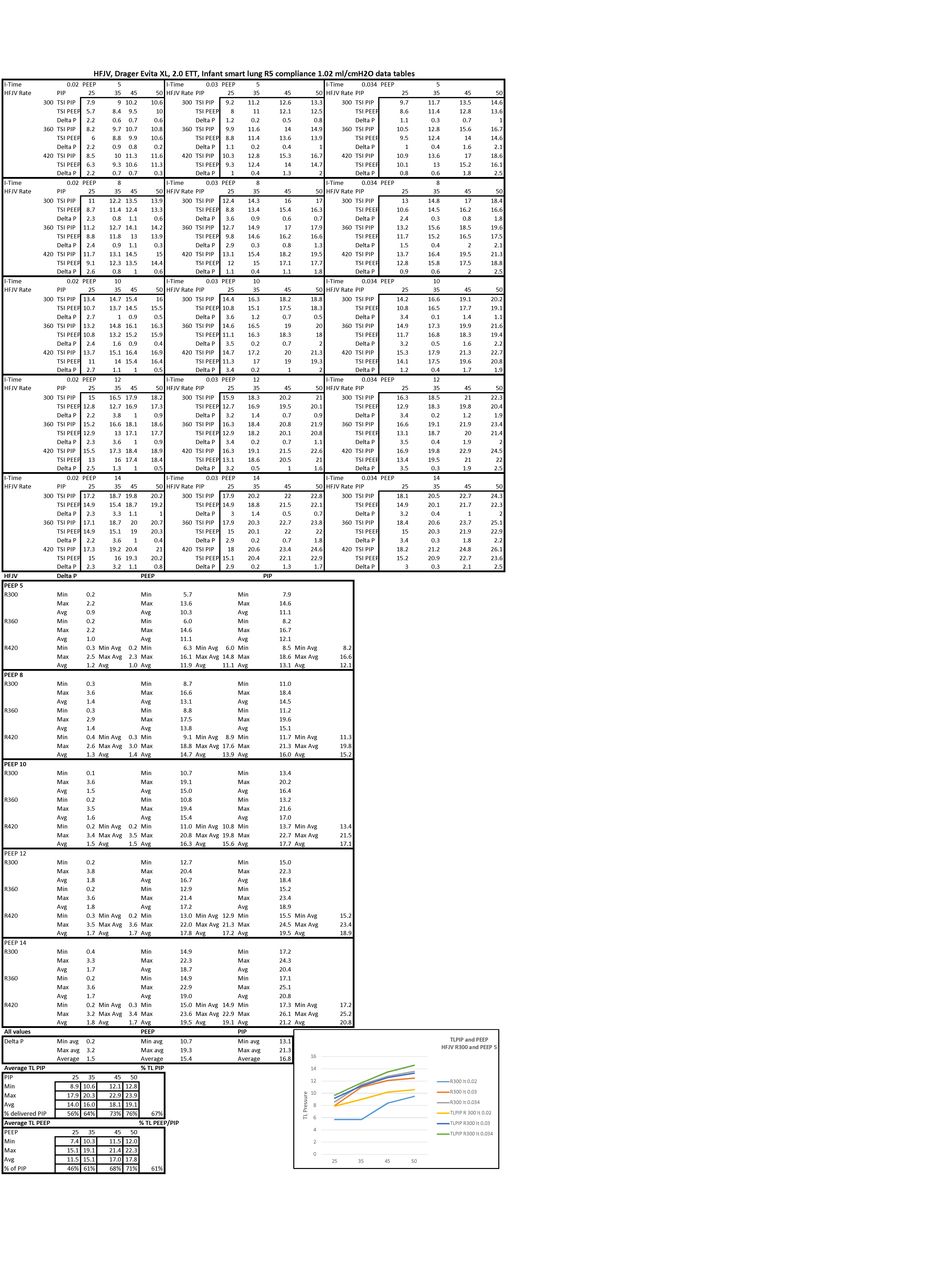
A HFJV and Drager Evita XL (XL) (Coppell, Texas) were prepared. A 2.0 ET tube was fitted with a 2.5 LifePort ETT adaptor. The ETT was connected to a TSI certifier FA Plus (Shoreview, Minnesota) and IMTmedical Smartlung Infant (Buchs, Switzerland). The TL was set on a compliance of 1.02 mL/cm H2O and resistance of 5. PIP and PEEP measurements were taken when stable. Changes to various settings were made on the HFJV and XL. Setting used were: Inspiratory time of .02, .03, .034 and PEEP of 5, 8, 10, 12, 14 and PIP 25, 35, 45, 50 and frequency of 300, 360, 420.
Results:
Across all values: PIP minimum average (min) 13.1, maximum average (max) 21.3 and PEEP min 10.7, max was 19.3 and ΔP min 0.2, max 3.2. TL PEEP average 62% higher than set. TL PIP average 67% lower than set.
Conclusions:
In our TL model significant attenuation and inadvertent PEEP was identified. Inadvertent PEEP increased as PIP increased, and ΔP decreased as PIP increased. Attenuation also increased with PIP increase. Further research with other lung models may be indicated as our results were limited to a fixed compliance with no leak.
Get full access to this article
View all access options for this article.