
Abstract
Background:
Carbon dioxide (CO2) is a potent regulator of cerebral blood flow (CBF). Preterm infants are particularly vulnerable to changes in CBF, due to impaired autoregulation of arterial vessels. The regulation of CO2 levels is important during the management of invasive mechanical ventilation in infants with RDS, as this value frequently changes. Hypercarbia, hypocarbia, and fluctuations in PCO2, are all associated with a variety of adverse events (AEs), many of which occur during the first 72 h of life. However, blood gases cannot be used for continuous monitoring, therefore we implemented a pilot of transcutaneous (Tcom) CO2 monitoring to improve management of this variable.
Methods:
We prospectively studied infants approximately 28 weeks gestation on invasive mechanical ventilation with Tcom CO2 monitoring. Demographic information was collected along with blood gas results extracted from the medical record. Data downloaded from the Tcom, including monitoring time (MT), CO2 values, date/time, heating power (HP; perfusion measure) and drift were matched with corresponding arterial or capillary blood gas results. Descriptive statistics were used to summarize patient characteristics and management issues, while the Pearson correlation coefficient was calculated to determine the strength of the linear relationship between blood gases and Tcom values (N=250 matched pairs).
Results:
The median age of all infants (N=12) was 24+4 d (23+6 — 25+6 d), with median weight 622.5 g (IQR 460-840 g), and 7 were male. Data show that the Tcom was ordered immediately post birth in only 2/12 infants. Two infants were placed on the Tcom approximately 2 days post birth; 3 at 3 days post birth; and 5 infants 4-days post birth. Data show above-average technical drift (4-6 mm Hg) during extended monitoring with the Tcom (average 25% of MT). In addition, all subjects experienced significantly high relative HP values (< -10 mW; average 30% of MT) without troubleshooting of probe placement. All subjects also experienced extended periods with the probe removed (average 30% of MT). The Pearson correlation coefficient results (r) = . 74 (P < .001).
Conclusions:
There were important issues related to sensor management which could have affected the bias of displayed Tcom to blood gas results. While the correlation between blood gases and the Tcom monitor was good, better management may improve this value as there were many outliers. Tcom monitoring is feasible in ELBW infants, but few were placed promptly on the monitor.
Figure 1. The residuals and fit plot of the correlation between transcutaneous CO2 and blood gas values.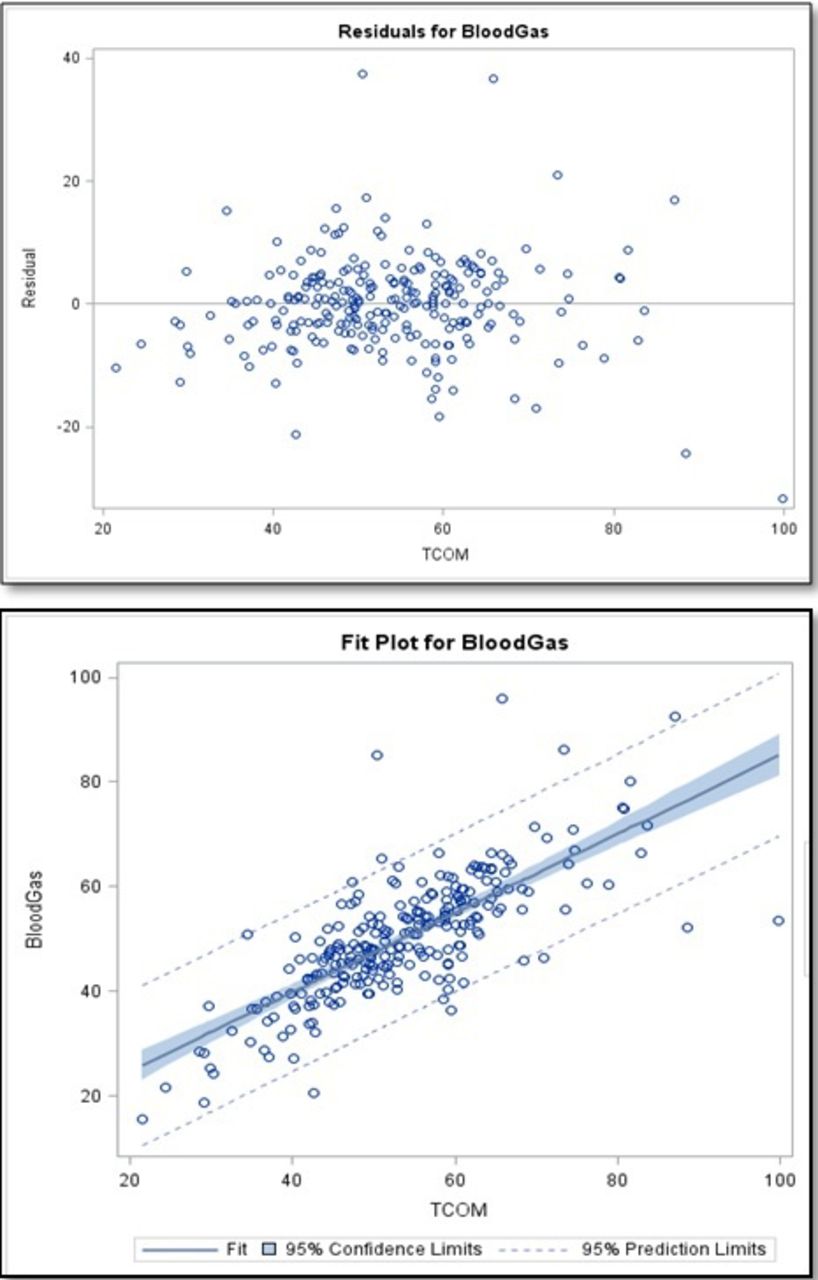
Get full access to this article
View all access options for this article.