
Abstract
Background:
Lung expansion therapy (LET) is often ordered after surgery to improve alveolar ventilation and reduce risks of postoperative pulmonary complications (PPC). The impact of LET at altering distribution of ventilation in non-intubated patients has not been described. The primary purpose of this study is to determine if there is a difference in dorsal redistribution of ventilation and incidences of PPCs when comparing Incentive Spirometry (IS) to EzPAP LET after upper abdominal surgery. Our a priori null hypothesis is that there are no differences.
Methods:
This IRB approved prospective randomized controlled trial enrolled adult human subjects who underwent upper abdominal surgery from January 2017 to April 2018. Subjects were allocated to receive LET with IS targeting predicted inspiratory capacity or EzPAP targeting 15 cm H2O TID on postoperative days (POD) 1-5. An electrical impedance tomography (EIT) device (Pulmovista 500; Draeger) was connected to subjects for a single LET session on POD 1, 3, and 5 to measure baseline changes in post-LET dorsal end-expiratory lung impedance (ΔEELI %). LET sessions with EIT included 2-min normal breathing, 3 breath cycles x 10 breaths, and 2-min normal breathing after breath cycle 3. The EIT device was removed after POD monitoring sessions but LET continued as scheduled. PPCs were screened until hospital discharge. Mann-Whitney U, x2, and Fisher's exact tests were applied as appropriate. Data are reported as count (n), percent, and median [IQR]. Alpha (2-tail) is < .05.
Results:
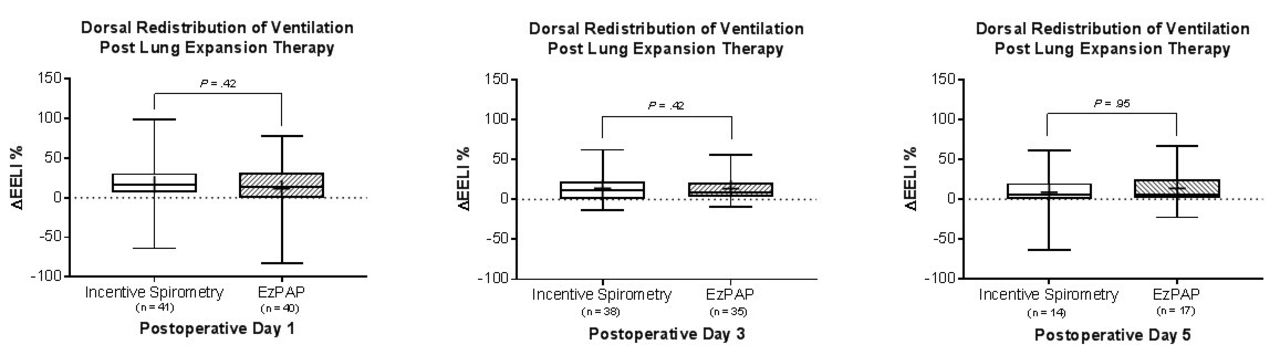
81 subjects were enrolled to receive IS (n=41) or EzPAP (n=40) LET. Groups were equal for descriptive characteristics such as age (62 [52-71] y), sex (57% female), BMI (28. 1 [24. 7-33.6]), ARISCAT PPC risk index (Score=41; intermediate risk) and comorbidities (P > .05). Whipple (38%) and hepatic resection (30%) accounted for the majority of surgical procedures. Protocol adherence (93% vs 89%, P = .39) and study dropout (4% vs 1%, P= .37) was similar between groups. Post-LET dorsal ΔEELI % increased for both groups, but median dorsal ΔEELI % for IS and EzPAP on POD 1 (16% vs 13%, P= .42), POD 3 (5% vs 6%, P= .42), and POD 5 (12% vs 9%, P= .95) was not significantly different. Hospital length of stay (4 d, P= .79) and incidence of PPCs (1% vs 4%, P= .19) was also similar.
Conclusions:
There is no difference in post-LET dorsal redistribution of ventilation or incidence of PPCs among adults who receive IS or EzPAP TID after upper abdominal surgery.
Get full access to this article
View all access options for this article.