
Abstract
Background:
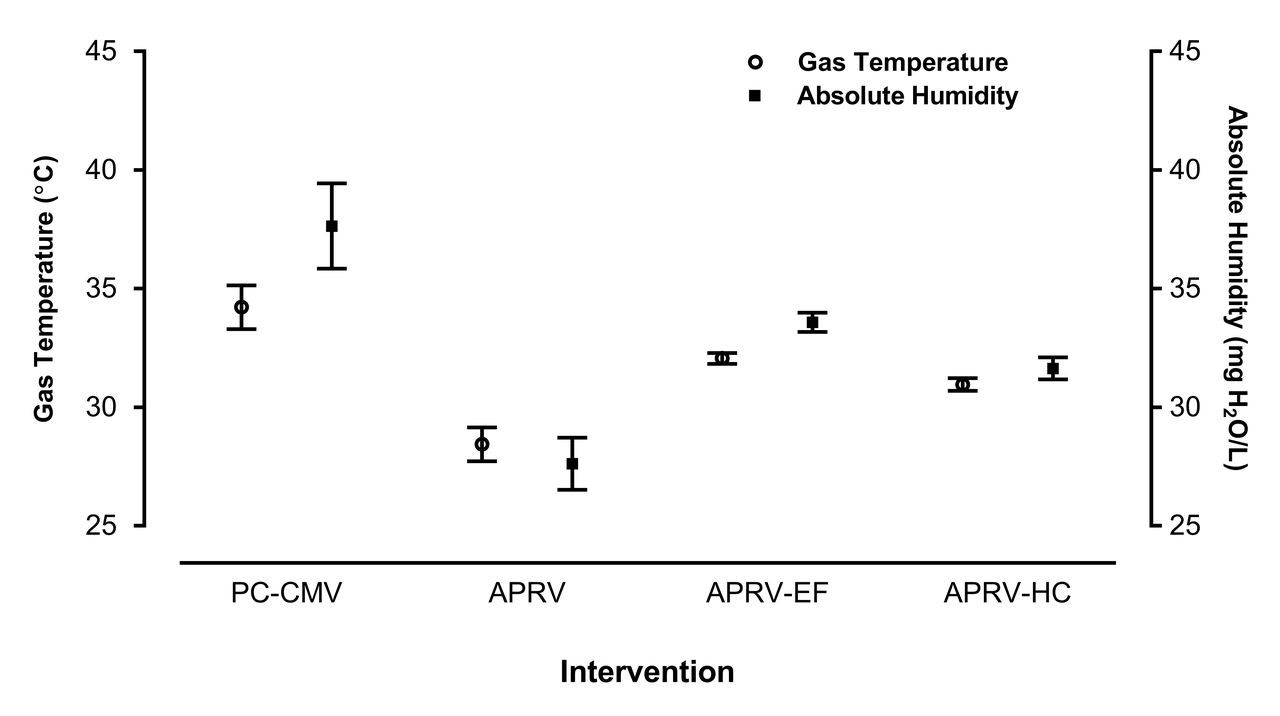
Heated humidifiers (HH) optimally operate with continuous or near-continuous flow. Standard HH performance requires gas temperatures (GT) 34°C - 41°C and absolute humidity (AH) 33 - 44 mg H2O/L. APRV incorporates a prolonged inspiratory phase creating no-flow conditions. Adjunct techniques used with APRV including external flow bled-in at 2 L/min or humidification augmentation with maximum humidity compensation may influence GT or AH. We sought to determine if APRV settings would provide acceptable levels of GT and AH using a pediatric ARDS lung model. Our null hypothesis is that during pediatric APRV, there is no difference in GT or AH when comparing PC-CMV with APRV, APRV using external flow (APRV-EF), and APRV with humidity compensation (APRV-HC).
Methods:
A conventional ventilator (Servo-i, Maquet) was equipped with an adult heated circuit (RT280, Fisher & Paykel) and connected to a HH (MR850, Fishery & Paykel). The ventilator was calibrated to the circuit with a pre-use check. A hygro-thermometer (Humidity Alert II, Extech) calibrated to NIST standards was placed at the circuit Y-piece. The ventilator circuit was connected to a test lung (ASL 5000, IngMar Medical) set to simulate a 10-year-old with ARDS (compliance 13 cm H2O L/s, resistance 30 mL/cm H2O, 6.0 ETT). Targeted lung protective ventilation settings are as follows: PC-CMV (frequency 20 breaths/min, PC 20 cm H2O, PEEP 12 cm H2O) and APRV (Phigh 30 Plow 0 Thigh 4 s Tlow 0.2 s). PC-CMV was initiated with heated humidity for 1 h. After each intervention change (PC-CMV -> APRV -> APRV-EF -> APRV-HC) a 10-min stabilization period preceded temperature and relative humidity measurements (every 5 min for 30 min) and AH was calculated from these measurements. Analysis was performed with a one-way ANOVA and post-hoc Tukey, as appropriate (SPSS, v24, IBM, Armonk, NY). Data was normally distributed for both GT and AH. Alpha (2-tail) set at .05.
Results:
There was a statistically significant difference in GT (P < .001) and AH (P < .001) between all interventions . The magnitude of the effect size was large for GT (w2 = .92) and AH (w2 = .91). Post-hoc analysis revealed a significant difference between all interventions in GT (P < .001) and AH (P < .001), except APRV-EF and APRV-HC groups in both GT (P = .51) and AH (P = .57).
Conclusions:
During APRV with low lung compliance, heating and humidification of inspired gas may not meet recommended standards for invasive mechanical ventilation regardless of adjunct techniques.
Get full access to this article
View all access options for this article.