
Abstract
Background:
Multi-Organ Dysfunction Syndrome (MODS) is common in ARDS. 'Cross-talk' injury between the brain and the lungs has been described, 1 but the mechanisms by which brain injury causes secondary lung injury appears better established compared to lung injury resulting in brain dysfunction. There is speculation that ARDS may cause secondary brain injury similar to what occurs during sepsis. 1 We inquired whether neurologic dysfunction, as measured by Glasgow Coma Scale (GCS), is present at ARDS onset in those without apparent neurologic injury, and whether it is related to ARDS severity or lung injury etiology.
Methods:
This retrospective study examined 1, 176 ARDS cases wherein GCS was measured within 24 hours prior to intubation and ARDS onset. Cases associated with primary neurologic injury or drug overdose were excluded. Subjects were classified by Berlin definition and primary ARDS etiology. Sequential Organ Failure Assessment (SOFA) scoring criteria was used to categorize neurologic dysfunction (GCS = 15, 14-13, 12-10, 9-6, <6). Data were expressed as median [IQR]. Continuous data were assessed using Kruskal-Wallis and Dunn's post-tests. Categorical variables were compared using Fisher Exact test. Alpha was set 0.05.
Results:
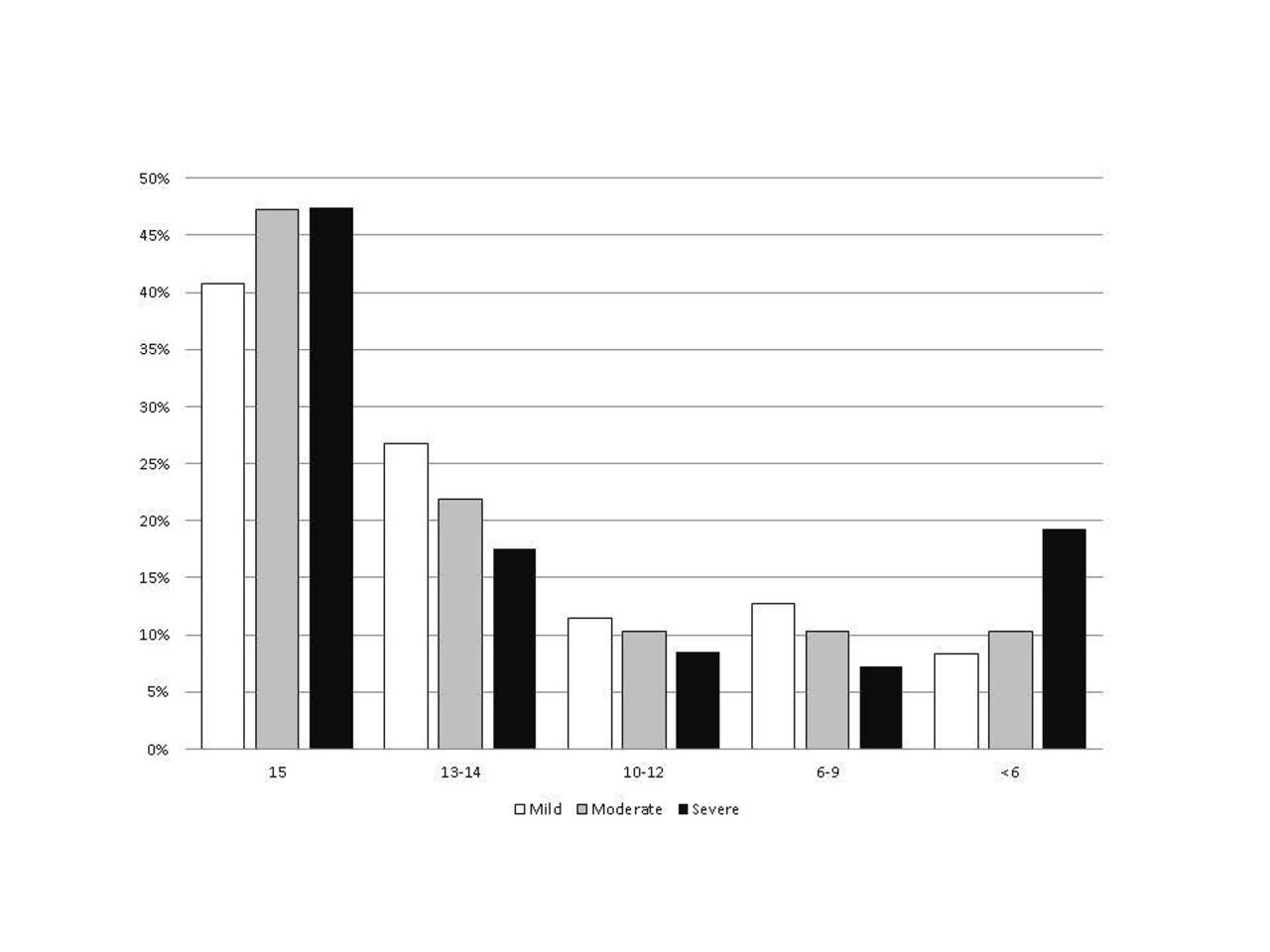
Less than 50% of subjects had a GCS of 15 within 24 h prior to ARDS recognition. The incidence of GCS <6 increased as ARDS severity increased from mild to severe (8, 10 and 19% respectively) (Fig). However, this was significant only between severe vs. mild (OR 3. 25 [1.64-6. 43], P = 0.0002) and severe vs. moderate (OR 1.94 [1.37-2.74], P < 0.0002). GCS was lowest in those with aspiration and highest in those with pneumonia: 11 [3, 15] and 15 [13, 15] respectively P <0.01. These etiologies represented 32% and 6% respectively of those with a GCS <6 compared to 9% when sepsis was the primary etiology. Moreover, GCS was not different in those with sepsis as a co-diagnosis versus without (14 [10, 15] and 14 [11, 15] P = 0.51 respectively).
Conclusions:
GCS was lowest in those with aspiration suggesting that neurologic dysfunction likely caused many ARDS cases via loss of upper airway reflexes. Contrary to speculation, 1 sepsis-induced ARDS was not associated with increased incidence of neurologic dysfunction.
Mrozek S, Constantin J-M, Geeraerts T. Brain-lung crosstalk: implications for neurocritical care. WWJCCM 2015;4(3):163-178.
Get full access to this article
View all access options for this article.