
Abstract
Background:
PaO2/FIO2 (P/F) ratio has been used as an effective means to assess both oxygenation status and respiratory distress syndrome (RDS) severity among pediatric patients as first noted in 1994 with Berlin criteria for RDS classification. However, P/F ratio requires an arterial blood gas in order to complete this calculation requiring sample collection by an invasive method to measure PaO2. With the emergence of noninvasive methods to measure oxygenation (ie, pulse oximetry) and a decrease in amount of arterial blood gasses drawn when compared to 20 years ago, this study was conducted to assess using SpO2/FIO2 ratio (S/F) as an option measure of oxygenation status to assess RDS severity and extubation readiness. However, definitive S/F ratio criteria has not been established for RDS severity category as is seen with P/F ratio and Berlin criteria.
Methods:
718 pediatric arterial blood gas samples from 32 PICU patients ranging in age from infant to 17 years of age were reviewed in this IRB approved study and P/F ratio was calculated for each sample. The average blood sample per patient was approximately 22 samples (n = 22.44) with a range of 1 to 59 samples per patient. Only collected SpO2 and SaO2 data values that were within ± 3% of each other from the electronic health record were used. All calculated values were entered into a spreadsheet and separated into RDS categories according to Berlin Criteria. Samples with PEEP were separated into 2 groups of PEEP < 7 and PEEP ≥ 7. Linear regression analysis was completed among RDS groups and also with samples that included PEEP.
Results:
S/F ratio showed the strongest positive relationship to P/F ratio when P/F ratio is <300 (r= 0.76). Using a 95% CI, S/F ratio increases, on average, 86 units for every 100-unit increase in P/F. In the two PEEP data groups, there was not a statistically significant difference in the slope of the best-fit lines (0.27 vs 0.25, P= 0.75). However, a high degree of overlap among RDS categories in S/F ratio exists when compared to P/F ratio suggesting that it is possible to have the same S/F ratio in all P/F ratio RDS categories.
Conclusions:
S/F ratio may be used as an effective measure of oxygenation in moderate to severe RDS categories. However, clinicians should exercise caution due to overlap across RDS categories. Since S/F ratio overlap is high in mild RDS to normal categories, it may not be an ideal assessment tool for assessing extubation readiness.
Overlap of SF ratio categories when compared to Berlin Critetria PF ratio RDS classification.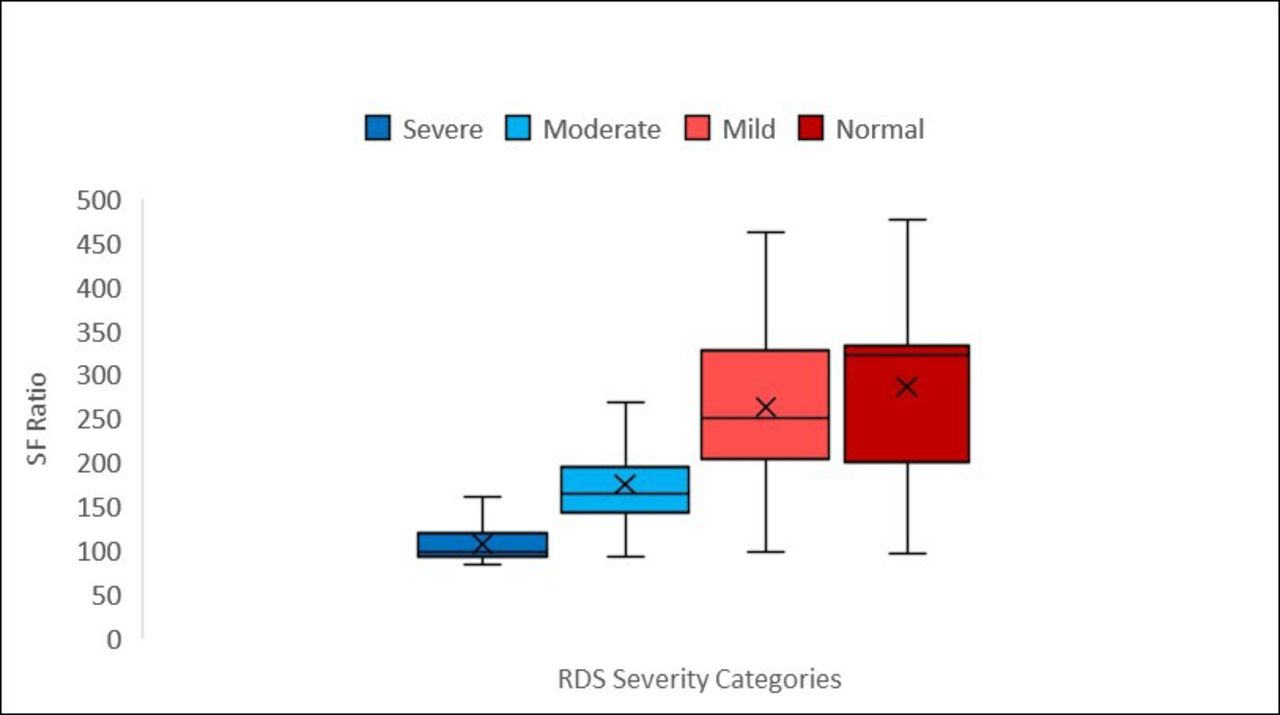
Get full access to this article
View all access options for this article.