
Abstract
Background:
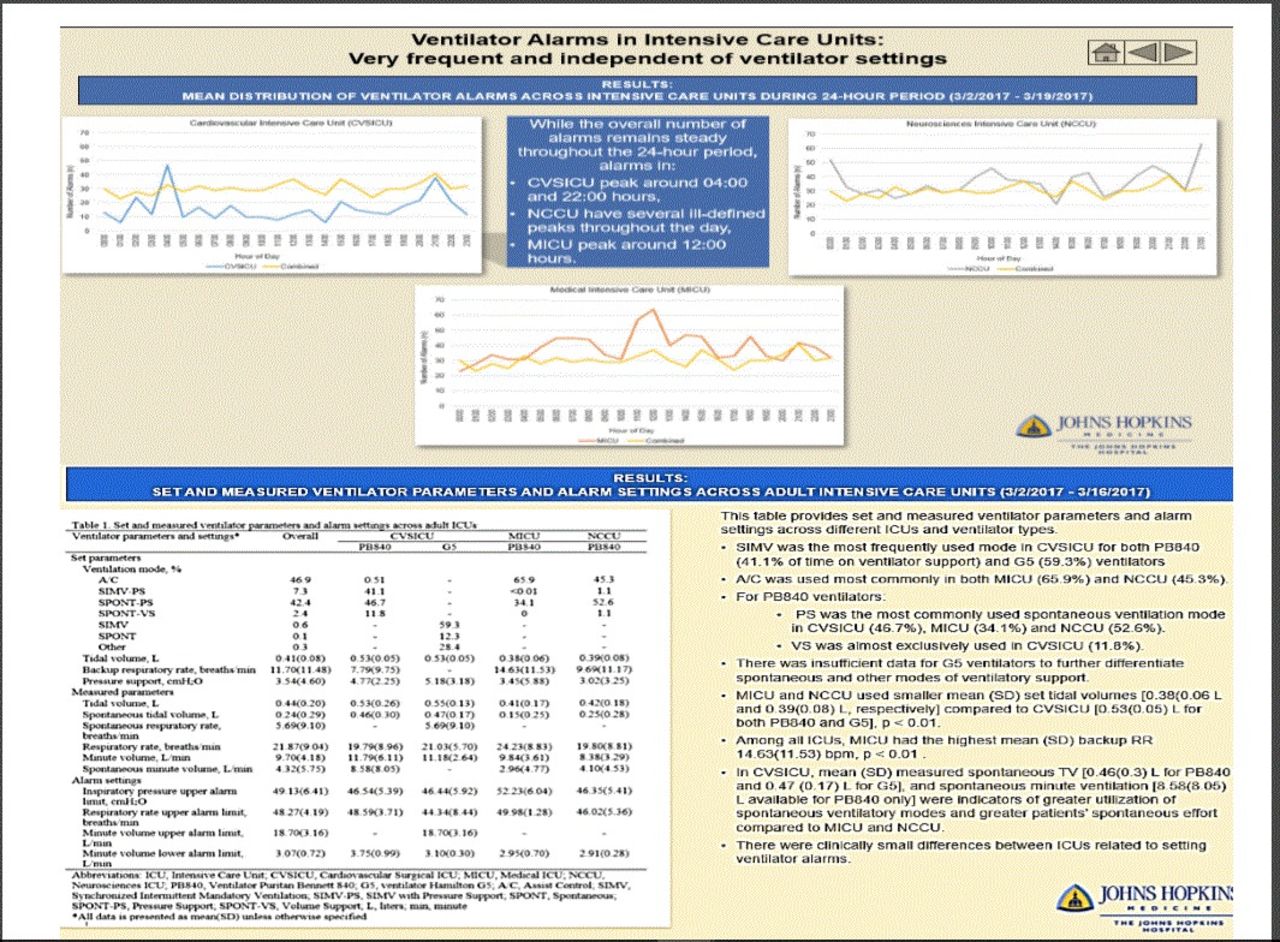
We evaluated the frequency, duration, and type of ventilator alarms occurring in adult intensive care units (ICUs) and examined determinants of alarm settings.
Methods:
This was a prospective observational study conducted in three ICUs — cardiovascular surgical (CVSICU), medical (MICU), and neurosciences critical care unit (NCCU) in a U. S. tertiary care university teaching hospital.
Results:
During 18 consecutive days, alarms were triggered 10, 933 times over 1, 555 ventilator-hours, averaging 7.0 alarms per ventilator-hour. Each alarm resulted in up to 8 notifications depending on alarm duration and acknowledgement by personnel. In the CVSICU and NCCU, initial alarm notifications via ventilator were duplicated via nurse call system, whereas in the MICU, a 60-s delay reduced duplicate notifications to 2.5%. Initial alarm conditions that did not resolve in ≤15 s triggered an additional notification cascade to respiratory therapists and nurses via hospital middleware. Forty percent of the alarms triggered such notification cascade, leading to 2.8 additional notification sequences per ventilator-hour for a total of 9.8 per ventilator-hour. The most common alarms were high inspiratory pressure (34. 2%), high breathing frequency (17.7%), and low expired mandatory tidal volume (12.9%). Alarm settings were independent of corresponding ventilator parameters for respiratory rate and minute volume in all ICUs.
Conclusions:
Ventilator alarms are highly prevalent, and notification systems amplify alarm burden by generating a cascade of messages about the same alarm. Prioritization of alarms varies between ventilator types owing to a lack of standardized classification. Alarm limits are arbitrarily set and not individually adjusted.
Get full access to this article
View all access options for this article.