
Abstract
Background:
The lack of high fidelity task trainers presents a barrier to implementing invasive diagnostic procedures. The complexity of new evidence based modalities, such as esophageal balloon monitoring, requires comprehensive training to diminish patient risk. The objective of this study is to determine whether creating a custom task trainer improves confidence and simulates the appropriate ventilator scalar waveform responses for accurate placement.
Methods:
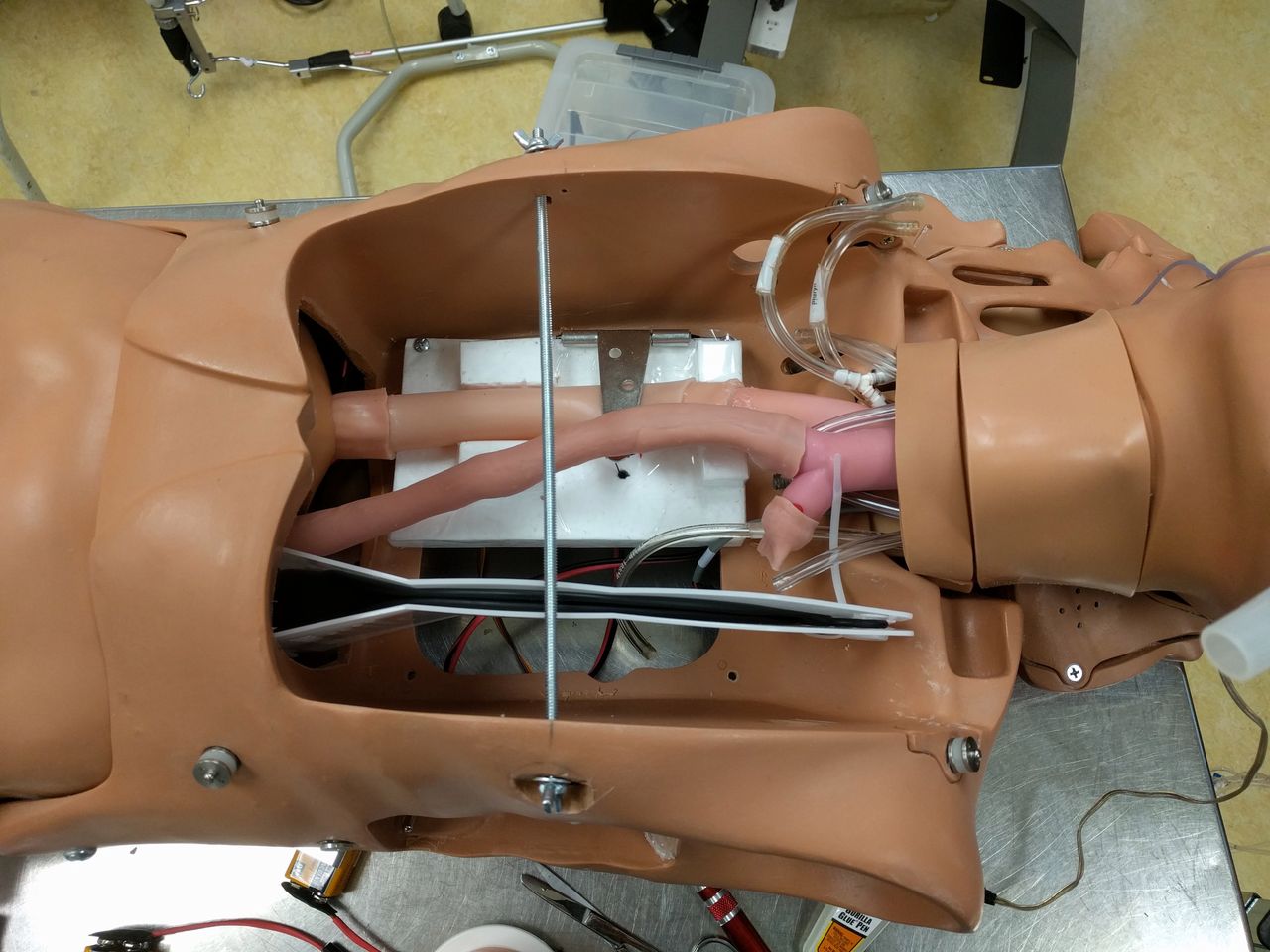
Sixteen hospital based registered respiratory therapists participated in the task training, with each performing three attempts at catheter placement. A non-functional, modified SimMan Classic was used as a chassis foundation. Extension tubing for the esophagus and trachea was created from silicone tubing. The stomach was created from a self-inflating bag and a one-way valve was placed at the top of the esophagus to maintain circuit pressure. A Y-connection was used to connect the trachea to the test lung and the back of the stomach to translate airway pressure to the esophagus. A servo control closed a hinge on the esophagus to create the cardiac oscillations in the correct location. Multiple 'dry runs' were conducted to ensure alterations to the SimMan Classic were able to produce cardiac oscillations for accurate catheter placement. Data collected from a post-training survey was used to determine if objectives were met.
Results:
Participant success rate for placing the catheter while observing the appropriate ventilator scalar waveform response mean (SD) 2.8 +0.4, or 93.7%. Limitations to the device include the inability to simulate inspiratory and expiratory maneuvers due to the one-way valve, which required the use of a secondary simulator for pressure interpretation and ventilator optimization. When participants were asked if the simulator increased confidence for performing this procedure, results showed 38% strongly agreed, 50% agreed and 12% somewhat agreed. When asked if the simulator was realistic enough to practice the skills necessary to accurately place the catheter, 50% strongly agreed and 50% agreed.
Conclusions:
There is a need for further investigation and development of simulators for the training of complex, invasive respiratory procedures. Future simulator versions to include the ability to perform inspiratory and expiratory maneuvers would be optimal for comprehensive training in esophageal balloon monitoring.
Get full access to this article
View all access options for this article.