
Abstract
Background:
Transnasal fiberoptic laryngoscopy (TFL) has revealed that laryngeal obstruction can hamper assisted ventilation. TFL may be considered invasive, and laryngeal ultrasound (US) could be a noninvasive alternative. The objective of this study was to investigate the feasibility of using laryngeal US to study laryngeal movements in healthy adult volunteers undergoing noninvasive ventilation (NIV) and to compare the observations with those of simultaneous TFL.
Methods:
In this cross-sectional study, 30 participants (19 females, age 22–65 y) underwent simultaneous video-recorded TFL and laryngeal US, breathing with and without NIV. Laryngeal US was repeated for anterior and both lateral approaches; the last 5 breaths from each assessment were analyzed. The participants rated discomfort using a numeric rating scale (NRS) from 0 (no discomfort)–10 (worst). Two blinded raters separately described and scored the TFL and laryngeal US recordings, and the findings were subsequently compared. The last 10 laryngeal US recordings were tested for interrater reliability.
Results:
All participants were successfully assessed using the anterior and both lateral laryngeal US approaches during NIV. Both techniques were well tolerated; 5/30 scored 0 on NRS for TFL and 22/30 for laryngeal US. The visualization rate for all recorded breaths was 99.1% for TFL compared to 81.7% for laryngeal US; overall concordance rate was 84.6%. The discordance rate for the TFL versus laryngeal US observations was 11.1% for vocal fold movements and 11.7% for aryepiglottic fold movements. Interrater reliability showed substantial agreement (0.71).
Conclusions:
Laryngeal US emerged as a feasible method to describe laryngeal movements during NIV, providing high-quality observations and high concordance with TFL.
Introduction
Noninvasive ventilation (NIV) is used to prevent and alleviate respiratory failure, thereby preserving both quality of life and survival. 1 The larynx is an essential gatekeeper for the lower airways and, therefore, important during NIV. In some persons, the larynx may act as a malfunctioning valve, especially when high positive pressures are applied. 2 This situation leads to obstructed air flow, which is a condition where NIV creates an induced laryngeal obstruction. NIV-induced laryngeal obstruction increases the inspiratory resistance and might reduce delivery of minute ventilation to the lungs. 3 , 4
Transnasal fiberoptic laryngoscopy (TFL) is the reference standard for upper-airway assessment and visualization of laryngeal movements. 2 , 5 Real-time TFL imaging has provided new important insights into the dynamic responses of the larynx when therapeutic pressures are applied to the airways. 6 –9 Given the vulnerability of NIV users, there is a significant interest in providing less invasive methods for visualizing laryngeal movements during NIV. Diagnostic ultrasound (US) equipment is widely available, and the required procedures are relatively easy to learn by trained health providers. 10 Laryngeal US has proven valuable in diagnosing vocal fold (VF) dysfunction following thyroid surgery and intubation in persons admitted to intensive care. 11 –13 Besides the diagnostic purpose in visualizing pathology, laryngeal US serves the purpose to monitor and evaluate functional responses. The novelty of our study lies in utilizing laryngeal US for functional assessment during an ongoing NIV treatment.
In order to consider implementing laryngeal US as a laryngeal assessment method for NIV users, its feasibility and validity need to be explored. Thus, this study aimed to investigate the feasibility of laryngeal US in observing and characterizing laryngeal movements during ongoing NIV in healthy adult volunteers and to compare the findings with those obtained by TFL.
QUICK LOOK
Current knowledge
Laryngeal obstruction can hamper ventilation in patients undergoing noninvasive ventilation (NIV). Transnasal fiberoptic laryngoscopy (TFL) is the reference standard for upper-airway assessment and visualization of laryngeal movements. There is growing interest in providing less invasive methods for visualizing laryngeal movements during NIV. Laryngeal ultrasound (US) has proven valuable in diagnostic purposes and might be a feasible method.
What this paper contributes to our knowledge
Laryngeal US was a feasible and well-tolerated method for upper-airway assessment and visualized laryngeal movements during NIV in 30 healthy participants. During NIV treatment, both vocal folds and aryepiglottic folds were of interest. Laryngeal US provided high concordance with TFL, and both expected and adverse movements were identified.
Methods
This experimental cross-sectional study involved healthy volunteers age 18 y and older. Participants were recruited from the staff at Haukeland University Hospital, Bergen, Norway, during spring 2022, exclusion criteria being a history of bronchospasm, pneumothorax, or pronounced nasal obstruction. The Regional Committee for Medical and Health Research Ethics in Northern Norway approved the study (ID: 2020–97615). All participants gave informed, written consent before inclusion. The study protocol is registered at ClinicalTrials.gov (NCT04586855). Details of the method have been published previously. 14
Sex, age, height, and weight of the participants were recorded. Spirometry was performed with Vyntus spirometer (Vyaire Medical, Mettawa, Illinois) according to European Respiratory Society guidelines. 15 , 16 Respiratory muscle strength was measured using a respiratory pressure meter (MicroRPM, Vyaire Medical); 17 plateau values (average of 1 s) of the maximum inspiratory (PImax) and expiratory (PEmax) pressures were reported. PImax was measured from residual volume and PEmax from total lung capacity. The measurements were undertaken with the participants in a seated position, and the highest values from 3 attempts were recorded.
The participants were assessed with TFL and simultaneous laryngeal US during 2 different interventions: breathing with and without NIV (VPAP Stellar, ResMed, San Diego) used in spontaneous mode. The participants were assessed in a seated reclined position. The laryngeal assessments were performed with 3 different laryngeal US probe placements, with approximately 1 min of breathing/placement (see Table 1).
The laryngeal assessment method with intervention and intervention name
Probe placement for lateral laryngeal ultrasound is shown.
US, ultrasound; TFL, transnasal fiberoptic laryngoscopy; NIV, noninvasive ventilation; Mode S, spontaneous mode; IPAP, inspiratory positive airway pressure; EPAP, expiratory positive airway pressure; B, baseline breathing without NIV.
Participant baseline characteristics
Data are presented as mean ± SD (range) or median (interquartile range).
P value estimated by Mann-Whitney U test for difference between females and males.
BMI, body mass index; PEF, peak expiratory flow; PImax, maximal inspiratory pressure; PEmax, maximal expiratory pressure; TFL, transnasal fiberoptic laryngoscopy; US, ultrasound; NIV, noninvasive ventilation.
Transnasal fiberoptic laryngoscopy
Participants were placed in a reclined position on an examination chair with the headrest inclined at a 40° angle and their necks slightly extended. A local anesthetic spray (0.1 mL of 4% lidocaine, Accord Healthcare, Middlesex, United Kingdom) was applied before the lubricated flexible laryngoscope (diameter 2.6 mm; ENF-V3, Olympus, Tokyo, Japan) was advanced through a modified full face mask (face mask for CoughAssist Ventilatory Circuit, Philips Respironics, Murrysville, Pennsylvania) into the nasopharynx until a satisfactory view of the larynx was obtained. The end of the laryngoscope was positioned just above the tip of the epiglottis, and the position was adjusted as required for optimal visualization of the glottic (the VFs) and supraglottic (aryepiglottic folds [AEFs]) structures. A physician adjusted the laryngoscope manually during the examination.
Laryngeal ultrasound
We assessed the larynx with 3 probe placements (see Table 1). The anterior laryngeal US imaging technique primarily visualizes the VF movements, 12 , 13 using the thyroid cartilage as the anatomical landmark to identify the VFs. The lateral laryngeal US imaging technique visualizes the arytenoid cartilage movements, considered a surrogate measure of VF movement, as the cartilages are attached to the lateral part of the VFs. 18 The purpose of a functional assessment during ongoing NIV treatment in patients in the hospital or at home formed the device model decision for laryngeal US. After application of US gel, the linear US transducer (frequency 5–10 MHz) of the portable US device (Vscan Air, GE Healthcare, Chicago, Illinois) was used in the 2-dimensional mode. First, the transducer was placed anteriorly and transversely over the middle section of the thyroid cartilage for imaging of the bilateral VFs. The participants were asked to phonate “eee” to identify targeted laryngeal structures before each assessment. Thereafter, the transducer was placed vertically 1–1.5 cm inside and parallel to the lateral border of the thyroid cartilage, along the oblique line. The transducer was placed laterally on both sides of the thyroid cartilage to observe both arytenoid cartilages separately and indirectly identify AEF movement. The transducer placement, depth, and gain were adjusted as required for optimal visualization of the targeted structures by a physiotherapist experienced in US. 14
Simultaneous recording of TFL, laryngeal ultrasound, NIV device panel, and air flow and pressure registrations
The TFL was visualized on a television screen, the US transducer signals on a portable mounted tablet (Galaxy Tab S7, Samsung, Seoul, South Korea) via Bluetooth, and the NIV device’s control panel was video-recorded by an external video camera (Sony SRG-300HW, Sony Computer Science Laboratories, Tokyo, Japan) for continuous visualization during the entire examination. Air flow and pressure curve registrations were used to couple the visual images to the inspiration and expiration phases (see Figure 1). All the sources were visualized via HDMI wires and Cam Link 4K (Corsair Memory BV, Almere, the Netherlands) to one screen with Open Broadcaster Software v.26.1.1, 64-bit for Windows. The software recorded all the simultaneous recordings as one video file and stored this on the research server, allowing retrospective investigation of the laryngeal movements during the procedures with each assessment method (Supplementary Video). To ensure adequate quality of the recordings, the complete setup was shown in real time during the entire procedure on a computer screen present in the same room and was always visible to all examiners.
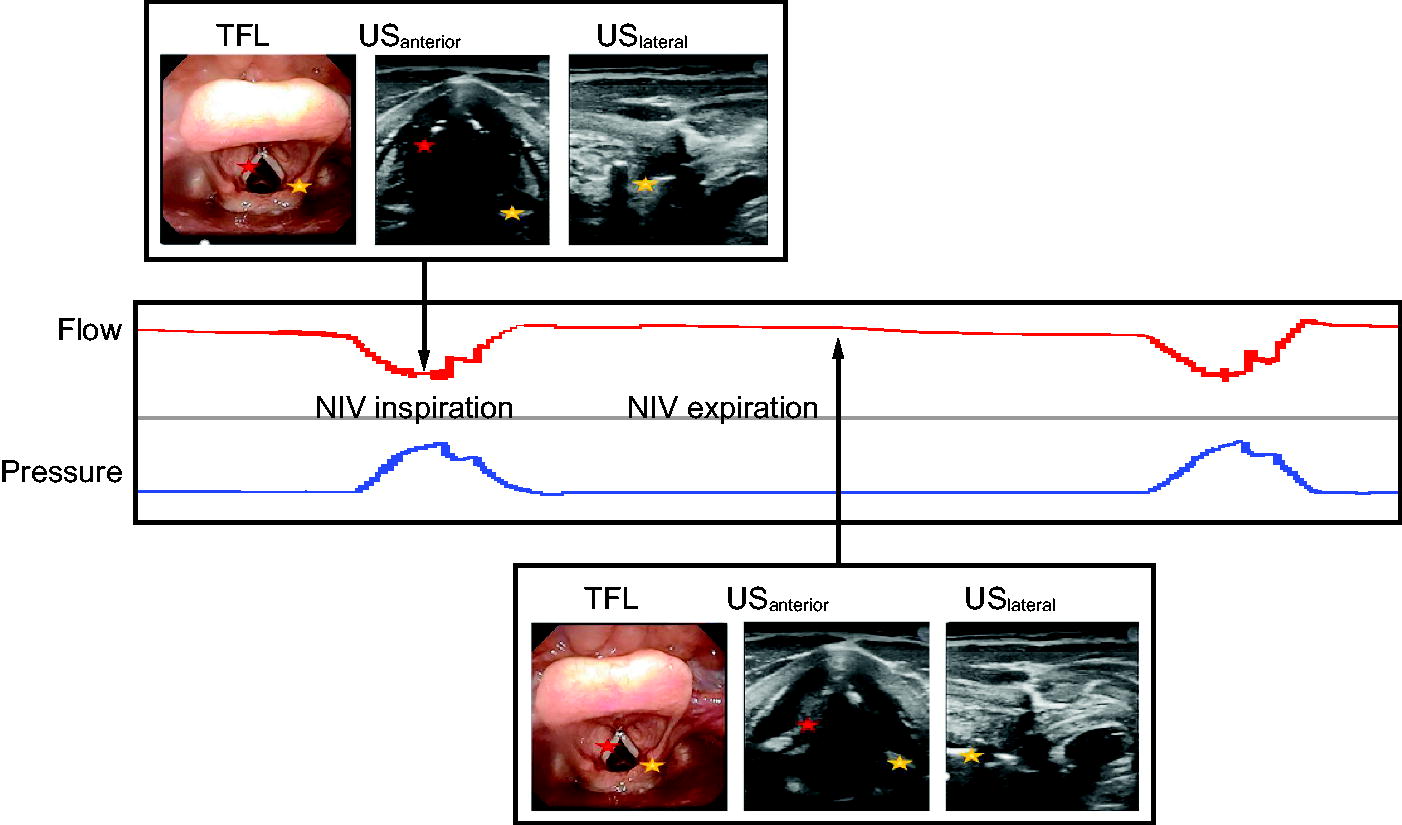
An illustration of the expected normal laryngeal movements observed during NIV with abduction at glottic and supraglottic levels during inspiration and adduction at both levels during expiration. Anterior laryngeal US technique visualizes both levels, and lateral laryngeal US technique visualizes the supraglottic level. Yellow star, aryepiglottic folds; red star, vocal folds; TFL, transnasal fiberoptic laryngoscopy; US, ultrasound; NIV, noninvasive ventilation.
Outcomes and assessments
The laryngeal US recordings were rated first by GN and AKB, followed by rating of the TFL recordings by TA and AKB. Both sets of recordings were assessed in real time and retrospectively in slow motion, with the recordings from the other method concealed during scoring. For the last 10 participants of the laryngeal US evaluation, the experienced observers’ interpretation was used (GN). We applied the assessment method used in Andersen et al 7 for evaluation of the TFL images, and this system was further adapted for laryngeal US evaluation. The final 5 breaths from each assessment were analyzed, resulting in a theoretical total of 890 respiratory cycles available for comparison.
First, the operator’s ability to visualize the targeted structures was assessed. We defined cases where the VFs or AEFs were visualized as assessable and cases where they were not visualized as non-assessable. For assessable cases from TFL and laryngeal US recordings, the laryngeal responses were characterized as either abduction or adduction of the VFs and the AEFs during inspiration and expiration. TFL served as the reference standard when comparing the observed laryngeal movements.
Further, the concordance and discordance was determined, referring to the extent of agreement between observations (concordance) and to the disagreement between observations (discordance) made simultaneously with laryngeal US and TFL. A numeric rating scale (NRS) of 0–10 was used to evaluate the study participants’ perception of the TFL and the laryngeal US examination separately, where 0 is not unpleasant at all and 10 is the worst imaginable discomfort. Interpretation of the laryngeal US observations from the first 20 participants was performed in a collaborative setting by the experienced (GN) and the novel US interpreter with only basic US skills (AKB). For the evaluation of the last 10 participants, the 2 raters scored separately, and interrater reliability was assessed as the degree of agreement between the 2 raters.
Statistical methods
Data were stored and processed in Stata v.17 for Windows (StataCorp, College Station, Texas). As this was an explorative study, power calculations were not performed, and the results were analyzed in a descriptive fashion. Baseline data are presented by means, SD, and ranges (min-max), and participants` perception are presented as median with interquartile range to avoid influence of possible outliers. Mean values were compared between males (n = 11) and females (n = 19) using Mann-Whitney U test. P values were 2 sided, and values below .05 were considered statistically significant. Categorical data were presented as frequency counts and percentages. Assessable participants were compared to describe the accuracy of laryngeal US, using TLF as reference. Visualization rate was calculated as the percentage of visible VF and AEF movements from the total number of movements during the inspiratory and the expiratory phases (combined in Table 3 and separately in Table 4), with and without the use of NIV. Assessability was given as numbers for inspiration and expiration (separately in Table 4 and combined in Table 5). The agreement between the methods was given as a ratio of concordant and discordant findings using all breath cycles that had been deemed assessable by both methods (Table 3) or the assessable cases (Table 5).
Visualization rate with transnasal fiberoptic laryngoscopy and laryngeal ultrasound during breathing with and without noninvasive ventilation
Data are presented as no./no. (%). The assessable respiratory cycles are divided into inspiration and expiration, each reported separately. The concordance rate refers to the extent of agreement in observations made simultaneously with laryngeal ultrasound compared to transnasal fiberoptic laryngoscopy.
no., number of probe placements; TFL, transnasal fiberoptic laryngoscopy; US, ultrasound; VF, vocal fold; AEF, aryepiglottic fold; NIV, noninvasive ventilation.
Laryngeal assessability and visualization rate for each assessment with transnasal fiberoptic laryngoscopy and laryngeal ultrasound during breathing with and without noninvasive ventilation
Some small differences between visualization rate during inspiration and expiration were observed due to the differing number of visualized breaths.
One participant not examined during this assessment.
TFL, transnasal fiberoptic laryngoscopy; US, ultrasound; INT, intervention; A, assessable; NA, non-assessable; %, the percentage visualization rate was calculated from 5 or fewer available breaths; NIV, noninvasive ventilation; B, baseline breathing.
Concordance between the inspiratory laryngeal movements as observed by transnasal fiberoptic laryngoscopy and laryngeal ultrasound during noninvasive ventilation
Data are presented as number per probe placements.
VF, vocal fold; AEF, aryepiglottic fold; TFL, transnasal fiberoptic laryngoscopy; US, ultrasound.
To evaluate the agreement between 2 US raters for each observed movement, Cohen kappa analysis was used. The interrater agreement was calculated as an intraperson analysis. For each participant, the observed movement for both laryngeal levels and both respiratory phases assessed with the 3 probe placements were scored by both raters and then compared. The kappa statistics was interpreted as follows: < 0, poor agreement; 0–0.20, slight agreement; 0.21–0.40, fair agreement; 0.41–0.60, moderate agreement; 0.61–0.80, substantial agreement; and 0.81–1.00, almost perfect agreement.
Results
All 30 participants (63.3% female) completed the NIV examination according to the protocol; the sample demographics and perception of the examination are presented in Table 2. The described setup resulted in a total of 858/890 respiratory cycles available for analysis without technical problems. The laryngeal US operator had to make continuous adjustments with the probe to maintain visualization of the targeted structures and incorrectly identified a structure as the AEF in one of the lateral assessments during NIV (NIV 3). One participant was examined only once during breathing without NIV before the protocol was completed.
Feasibility of the laryngeal assessment methods
The total visualization rates for all breaths in both respiratory phases during breathing with NIV were 99.1% with TFL and 83.9% with laryngeal US and without NIV 94.3% with TFL and 88.2% with laryngeal US. The concordance rates for TFL and laryngeal US were 84.6% of breaths with NIV and 83.9% of breaths without NIV. The visualization rate was slightly higher for the AEFs than for the VFs (for details, see Table 3). During breathing with NIV, the video recordings were assessable for all participants with both laryngeal assessment methods, while without NIV all participants were assessable with TFL and at least in one view in 29/30 with laryngeal US. Three participants were non-assessable with an anterior view but were assessable with both lateral views. The remaining were assessable with at least one lateral view (NIV 2 or NIV 3). During anterior laryngeal US, the operator identified not only the VF but also the AEFs in 22/27 participants. The visualization rate was generally lower for male participants during anterior view (see Table 4 for details).
The participants` perception of the 2 laryngeal assessment methods was described as tolerable, with a median NRS score of 1.25 (1–3) for TFL and 0 (0–1) for laryngeal US. However, 5/30 perceived no discomfort using TFL compared to 22/30 by laryngeal US (Supplementary Table S1). The participants reported a median NRS score of 1 (1–3) for the application of NIV treatment.
Laryngeal findings during NIV
This was a methodological study, and assessing the quality of the laryngeal movements per se was not an objective. Nevertheless, some heterogeneity in the laryngeal responses was noted, some of which are considered adverse (NIV-induced laryngeal obstruction), such as inspiratory VF and/or AEF adduction, the latter occurring somewhat more frequently than the former.
During inspiration, the concordance rate for the movement of the VFs was 88.9%. Visualization of the AEFs was possible with all the 3 probe placements, and the total concordance rate for the laryngeal movement was 88.3%. The concordance rate for NIV 1 was 90.9% (in one participant laryngeal movements were interpreted as adverse), 88.8% for NIV 2 (in one participant laryngeal movements were interpreted as adverse), and 85.7% for NIV 3 (2 participants with adverse laryngeal movements) (see Table 5 for details).
During expiration, the concordance for the observed movement by the laryngeal assessment methods during NIV 1 for the VFs was 23/27 (concordance rate 85.2%) and 19/22 participants for the AEFs, 22/27 participants during NIV 2, and 22/28 participants during NIV 3. Concordance was reached in 63/77 (concordance rate 81.8%) probe placements for AEFs.
Interrater reliability for laryngeal ultrasound evaluation in 10 participants
The degree of agreement in the interpretation between assessors varied for each individual participant (Supplementary Table S2). Summarized agreements for observed movements for the 10 participants are 84.6%, κ = 0.71 (CI 0.68–0.74).
Discussion
Laryngeal US is a feasible method to visualize and assess laryngeal movements of interest during NIV. All volunteers were assessable with laryngeal US; the method provided high visualization rates and high concordance with TFL. Both assessment methods were well tolerated, with 5/30 of the participants perceiving no discomfort with TFL compared to 22/30 with laryngeal US. There were substantial levels of agreement between the 2 methods despite some variability in the interrater interpretation of laryngeal US. Thus, laryngeal US may serve as an alternative assessment method for investigating cases where treatment failure is suspected to be of laryngeal origin.
Laryngeal ultrasound feasibility
All participants were successfully assessed using either anterior or lateral laryngeal US. Whereas this study represents the first investigation of laryngeal US as a functional assessment of the larynx during NIV or other treatment interventions, previous studies have explored the visualization rate in diagnostic VF mobility in persons undergoing thyroid surgery. 19 –21 Swallowing is also a functional task, but studies in this field monitor movements of other structures than VF and/or AEF. 21 A systematic review reported varying rates of non-assessability with cases linked to calcification of the thyroid cartilage, predominantly observed in male subjects. 19 In response to this challenge, a combined approach to the study method was adopted, incorporating both anterior and lateral views. The visualization rate during NIV was generally high, a finding consistent with previously reported visualization rates in various diagnostic US studies of the larynx incorporating combined approach, 20 –23 both preoperative and postoperative laryngeal US assessments. 20
Our study population resembled previous research cohorts, which primarily included a higher proportion of females and younger males. 22 , 23 Previous research has indicated that older age and male sex are factors associated with reduced visualization of the VF due to the thyroid cartilage shape and calcification. 10 , 19 , 23 A greater difficulty in visualizing males with the anterior view compared to the lateral views was encountered, evidenced by a lower visualization rate for anterior probe placement. Further, a high body mass index (BMI) has been reported to impact visualization, particularly in terms of sensitivity and specificity. 22 All participants enrolled in this study exhibited normal BMI, precluding an assessment of the potential impact of BMI on laryngeal visualization during NIV.
As previously stated, our study was developed based on the knowledge that the lateral laryngeal US technique detects the movement of the arytenoid cartilage as a surrogate measure of VF movement. 18 From the diagnostic field of VF mobility, the structures of interest (VF or AEF) do not appear to be given clinical importance for VF mobility assessment. 24 However, these structures might not respond similar to positive pressure. 6 –8 As demonstrated in this study, the movements of VFs and AEFs do not always respond similarly during NIV. Therefore, during question of NIV-induced laryngeal obstruction, the movements at both the glottic and supraglottic levels are of interest since both structures might create NIV-induced laryngeal obstruction. Methodologically, our study differs from those investigating VF movement pre and post surgery including the use of combined laryngeal US views and concurrent TFL. Most importantly, the laryngeal assessment methods in our study aimed to evaluate functional dynamic movements as responses to potential inducers of laryngeal obstruction rather than as structural abnormalities to obtain correct diagnosis. The examination posed several challenges due to the inherent flexibility of the larynx and the multidirectional movement of the examined structures in both sagittal and transverse planes during NIV. As a result, continuous adjustments of the laryngeal US probe and laryngoscope were necessary to maintain good visual access. Both assessment methods were well tolerated by the participants. Laryngeal US was highly tolerated with a majority of the participants experiencing no discomfort at all. In contrast, only 5 of 30 reported the same for TFL. One extreme outlier (rated TFL to 0 and laryngeal US to 9) was identified. In a study conducted by Wolff et al, 23 a higher proportion of subjects preferred laryngeal US over TFL, with only 10 of totally 230 expressing a preference for TFL. It is important to note that all our participants received local lidocaine spray anesthesia, while Wolff et al 23 administrated anesthesia if required. In the studies by Andersen 6 , 8 using mechanical insufflation-exsufflation during TFL, the subject`s experience was not explicitly assessed, but none of the participants participating in the first assessment session refused to participate in the follow-up study due to discomfort from the TFL.
Concordance of the 2 laryngeal assessment methods
In our comparative analysis of the 2 laryngeal assessment methods, the same methodology as previously described for assessing VF mobility 11 , 22 was adopted. In this healthy population, only normal laryngeal movements during NIV, that is, abduction of the VF and AEF during inspiration and adduction of the VF and AEF during expiration, were expected; and therefore, validation of laryngeal US in terms of detecting abnormal laryngeal movements such as NIV-induced laryngeal obstruction was not possible. Instead, we compared observations from the reference standard TFL with observations from using the laryngeal US, data expressed as degree of concordant and discordant findings and rates. Nevertheless, among some of the participants assessed, we observed adverse laryngeal movements, that is, adduction of the VF and AEF during inspiration. Discordant findings regarding adverse laryngeal movements were observed at both levels with both anterior and lateral views, though in small numbers. Importantly, the laryngeal US method was able to detect adverse laryngeal movements with the same level of agreement with TFL as observed for expected movements. This is important, as such adverse movements would be the target for laryngeal US in future assessments of clinical scenarios of unsuccessful treatment with NIV. Our current understanding of the demographics and dynamics of NIV-induced laryngeal obstruction is limited. Future studies could benefit from employing noninvasive methods, such as laryngeal US, to further investigate these aspects.
Reliability
In the present study, a single experienced operator performed all laryngeal US assessments, while 2 independent raters interpreted the recorded laryngeal US assessments. This approach allowed for retrospective evaluation and enabled us to assess interrater reliability for the last 10 participants. In health research, both kappa and percent agreement are important metrics; however, a more restrictive judgment of the interpretation than Cohen’s original level is proposed. 25 Interestingly, the experienced assessor labeled more participants as non-assessable compared to the novel interpreter (2 vs none). Furthermore, there was no agreement regarding individual kappa interpretation for 3 of 5 male participants.
The existing literature offers limited evidence regarding the learning curve for accurate assessment. 19 , 20 The accuracy of laryngeal US relies heavily on the quality of assessment of the operator. 20 Like in our study, one operator has usually performed the assessment, and the operator’s experience may differ from novice to highly experienced. 20 Kandil et al 22 found no improvement in accuracy with increasing experience, and another study has suggested that individuals with only basic diagnostic US knowledge can perform laryngeal US and identify VF immobility (family members). 26 However, one study reported that a novel laryngeal US (surgical residents) assessor achieved proficiency after the seventh examination and demonstrated accurate assessment after 40 examinations. 27 Their conclusion was not based on diagnostic accuracy and visualization rates but reduction in time duration for completing the examination. The present study indicates that basic US skills and knowledge apply for laryngeal US used as a functional assessment during NIV.
The primary strength of this study lies in its contribution to the understanding of a challenging clinical problem, that is, evaluation of a noninvasive assessment method for objective and verifiable examination of laryngeal function during NIV. However, upper-airway challenges during NIV often appear during sleep; and therefore, awake laryngeal assessment evaluation during ongoing NIV in healthy participants might not fully reflect laryngeal responses to positive pressure during sleep or during respiratory distress. Further investigation of the TFL and laryngeal US methods in NIV users is necessary to establish potential clinical benefits. A further limitation was the relatively small cohort, which complicated statistical handling. Moreover, the assessments of interrater reliability were based on a subset of only 10 examinations. The generalizability of the results might be affected using only one laryngeal US operator who was highly experienced in lung point-of-care US.
NIV plays a crucial role in supporting persons with respiratory failure. However, the application of NIV can be challenging, as the larynx responds heterogeneously to positive pressures, potentially leading to NIV-induced laryngeal obstruction and treatment failure. 28 To optimize NIV, individually tailored pressure and air-flow settings require assessment methods for evaluating NIV-induced laryngeal obstruction. Laryngeal US holds the potential to offer valuable clinical insights and guide clinical decision making in subjects depending on NIV. However, it is essential in future investigations to involve real NIV users. Our findings suggest that inclusion of both anterior and lateral laryngeal US probe placements is valuable, whereas inclusion of both lateral views seems less critical.
Conclusions
Laryngeal US is a noninvasive, well-tolerated, and easily accessible examination tool that enables comprehensive assessment of laryngeal function, both at the glottic and supraglottic levels during NIV. This method can serve as a laryngeal assessment tool to investigate cases where failure of NIV to perform as expected is suspected to be of laryngeal origin.
Footnotes
Acknowledgments
The authors thanks the study participants for their participation in this study (GE Healthcare, Australia and MediQuip, Australia). Thanks to the Norwegian Advisory Unit on Home Mechanical Ventilation and Bergen ILO group, Haukeland University Hospital, Bergen, Norway, for providing technical and scientific support. We are very grateful to physiotherapist Haakon Kvidaland and medical photographer Thor-Andre Ellingsen for valuable help with technical setup and support with the figure.
Author Disclosure Statement
Dr. Ntoumenopoulos discloses relationships with medical ultrasound companies that provide in-kind support with ultrasound equipment for training courses. Dr. Clemm discloses a relationship with Global Initiative for ILO. Dr. Andersen discloses a relationship with Breas. The remaining authors have disclosed no conflicts of interest.
Ms. Brekka presented part of this work at the 4th International ILO Conference, held June 15–17, 2022, in Bergen, Norway.
Funding Information
This study received funding from The Norwegian Advisory Unit on Home Mechanical Ventilation, Western Norway Health Authorities, Haukeland University Hospital, Bergen, Norway; and Helse Vest, Department of Thoracic Medicine, Haukeland University Hospital, Bergen, Norway.
Supplementary Material
Supplementary Video
Supplementary Table S1
Supplementary Table S2