
Abstract
Background:
CPAP benefits preterm infants with respiratory distress, including reduced bronchopulmonary dysplasia (BPD) incidence, surfactant use, and extubation failure. Successful CPAP weaning also promotes oral feeding. However, there is no consensus on the optimal weaning of CPAP in neonates. This study aimed to determine the effects of CPAP weaning guideline implementation on neonatal outcomes.
Methods:
CPAP gradual pressure weaning guidelines were implemented in the Penn State Children’s Hospital neonatal ICU in 2020. We included baseline data from infants (epoch 1) before guideline implementation in 2018–2019. We included infants (epoch 2) after implementing the guidelines during 2020–2021. The inclusion criteria were infants < 32 weeks gestation with CPAP support. Adherence with the CPAP weaning guidelines was the primary process measure. Primary outcome measures included successful CPAP wean on the first attempt. Balancing measures used were total days on respiratory support and hospital length of stay.
Results:
One hundred ninety-five infants were included in this study, 95 infants in epoch 1 before guideline implementation and 100 infants in epoch 2 after implementing guidelines. Infants in the 2 epochs were similar in median gestational age at 29 weeks versus 30 weeks (P = .47) and were similar in median birthweight at 1,190 g versus 1,130 g (P = .73). After implementing weaning guidelines, the successful weaning off CPAP improved from 9.5% to 54% (P < .001). The total days needed to achieve full oral feeds decreased by 7 d (29 median d vs 22 median d, P < .001). The BPD incidence was not significantly different between the 2 epochs at 17% versus 16%, P = .87. There was no difference in total days of respiratory support, total length of stay, the number of infants discharged on home nasogastric feeding, and demographic variables.
Conclusions:
The implementation of the bubble CPAP weaning guideline improved the successful weaning of CPAP and promoted oral feeding in preterm infants.
Introduction
Nasal CPAP is a simple and noninvasive method of providing ventilatory support to preterm infants with respiratory distress. 1 The use of nasal CPAP is associated with benefits such as reduction in respiratory failure, mechanical ventilation, and mortality. 1,2 Furthermore, it has been shown that nasal CPAP decreased the use of surfactant in very preterm infants < 28 weeks gestational age (GA). 3 Nasal CPAP also improves lung growth and alveolar recruitment with the maintenance of functional residual capacity in the alveoli, thereby reducing extubation failure. 4 –7 Another study showed that, over 16 y, the introduction of nasal CPAP bundles reduced the incidence of chronic lung disease, particularly bronchopulmonary dysplasia (BPD). 8
Associated risks with nasal CPAP use in preterm infants include increased incidence of pneumothorax, nasal trauma, 9 and possible intraventricular hemorrhage. 10 Conversely, premature or ad hoc nasal CPAP weaning may lead to atelectotrauma, apnea, prolonged oxygen exposure, and increased invasive ventilation support. 5,11,12
Therefore, there is a need for evidence-based practice guidelines for nasal CPAP weaning in neonatal ICUs (NICUs). Limited data and a lack of consensus among medical providers make it challenging to determine the optimal weaning process or timing for nasal CPAP in preterm infants. 13 Based on a systematic review 11 and 2 randomized trials, 14,15 we designed the nasal CPAP weaning guidelines to include predetermined postmenstrual age and weight at the time of weaning to promote successful weaning at the first attempt. This practice ensured that preterm infants would benefit from nasal CPAP by preventing premature ad hoc weaning. Thus, we implemented nasal CPAP weaning guidelines in Penn State Children’s Hospital, a single-center, level IV NICU, in 2020. This study aimed to establish whether the implementation of a nasal CPAP weaning guideline would lead to a higher success rate in weaning infants under 32 weeks GA from nasal CPAP on the first attempt over a 2-y period.
QUICK LOOK
Current knowledge
The benefits of CPAP for preterm infants with respiratory distress include reduced incidence of bronchopulmonary dysplasia, surfactant use, and extubation failure. Whereas there are many benefits, premature or ad hoc nasal CPAP weaning may lead to atelectotrauma, apnea, prolonged oxygen exposure, or increased invasive ventilation support. Currently, there is no consensus among neonatalologists regarding optimal weaning or timing of CPAP.
What this paper contributes to our knowledge
Implementing guidelines for weaning preterm infants off nasal CPAP based on predetermined age and weight criteria and utilizing a gradual CPAP weaning method increased the success rate of weaning during the first attempt. Furthermore, there was an increased incidence of achieving full oral feeds sooner.
Methods
Study population
A quality improvement study was conducted on preterm infants born < 32 weeks of gestation at Penn State Children’s Hospital between 2018–2021. The study included preterm infants born at a GA of ≤ 32 weeks who were admitted to the NICU between 2018–2021 and required nasal CPAP. This included infants who were initially intubated and then switched to nasal CPAP, as well as those who were never intubated and used nasal CPAP. Those preterm infants who were transferred to outside hospitals during the stay, with congenital heart anomalies, tracheostomies, or other complications such as bilateral renal dysplasia or gastric perforation, were excluded from the study. Epoch 1 included infants before nasal CPAP weaning guideline implementation in 2018–2019. Epoch 2 included infants after implementing the guidelines in 2020–2021. The 2 epochs were selected so that sample sizes between the 2 groups were comparable.
Intervention
Epoch 1 consisted of preterm infants treated with CPAP (Infant Flow, Vyaire Medical, Mettawa, Illinois) with nasal interface (Infant Flow, Vyaire Medical) and ad hoc weaning with sudden discontinuation of CPAP. In January 2020, bubble CPAP (Fisher & Paykel, Auckland, New Zealand) system with its FlexiTrunk nasal interface (Fisher & Paykel) and CPAP weaning guidelines were implemented in the NICU. Predetermined weaning criteria (Fig. 2), along with stability and failure criteria, were used to determine eligibility, stability, failure, and success of weaning. The gradual weaning protocol was initiated once the infants met the criteria at 32 weeks postmenstrual age and 1,600 g of weight at the time of weaning. The gradual weaning was initiated when stability criteria were met at CPAP 5 cm H2O and FIO2 0.21. Then, the subjects were weaned to 4 cm H2O for 24 h and then to room air. If the subjects failed the trial, they were placed back on CPAP 5 cm H2O. The next weaning attempt was made after a minimum of 1 week once the stability criteria were met again. The successful nasal CPAP wean was defined as an absence of increased work of breathing (persistent tachypnea, marked retractions), apneic episodes, or any bag-mask ventilation on room air without respiratory support for 7 d. Mild desaturations were treated with low-flow nasal cannula as needed. The nasal CPAP weaning guidelines were available to the clinical team and the nursing staff at the subject’s bedside.
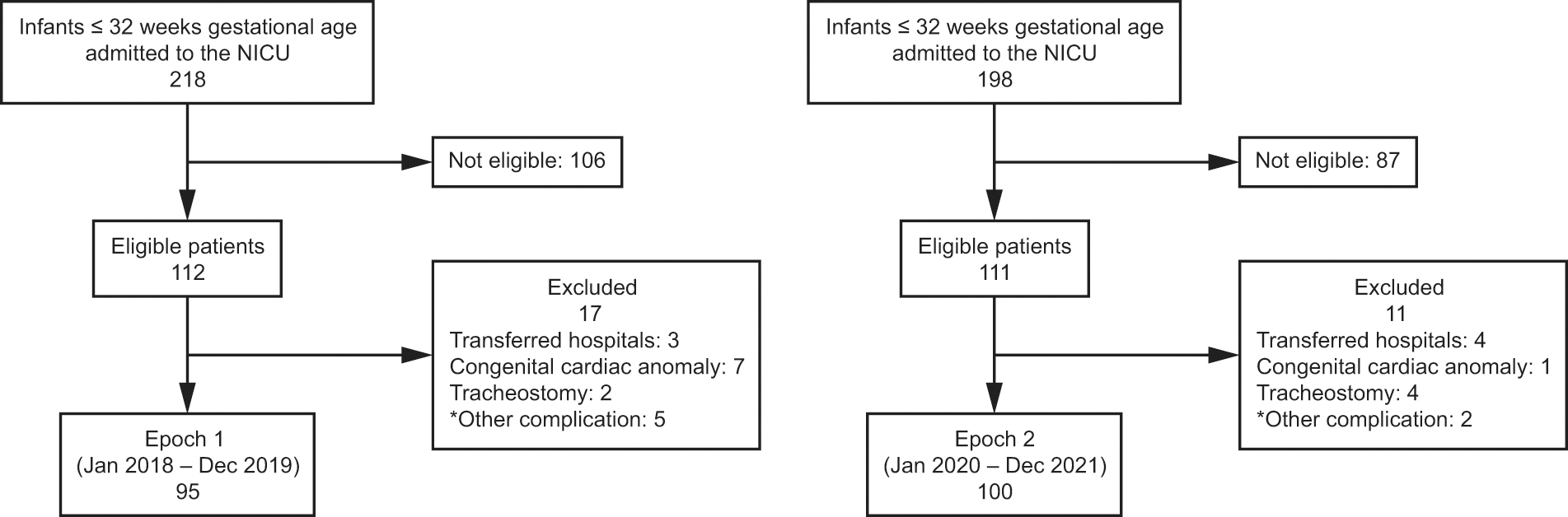
Flow chart. *Other complications include neurologic abnormality, congenital malformation, re-intubation for surgery, and death. NICU, neonatal ICU.

CPAP weaning criteria, stability criteria, failure criteria, and weaning protocol.
Quality improvement study
The quality improvement study was conducted from 2020–2022 and included 4 Plan-Do-Study-Act (PDSA) cycles. A group of health care professionals formed a task force to determine how to improve nasal CPAP in the NICU. The task force consisted of a neonatologist, a neonatal-perinatal medicine fellow, a nurse practitioner, a nurse educator, and respiratory therapists (RTs). They conducted a thorough literature review and developed an implementation plan and a weaning guideline. The task force presented the topic and their draft guideline at a neonatology division meeting to receive feedback.
Once the guideline was implemented, the clinical team consisting of the provider, bedside nurse, and RT performed assessments for weaning as per the guidelines and implemented the wean. The specific, measurable, attainable, realistic, and time-bound (SMART) aim of this study was to determine whether implementing a nasal CPAP weaning guideline would improve the successful weaning of nasal CPAP on the first attempt in a 2-y period in infants < 32 weeks of GA.
Change concepts
The primary drivers were the implementation of bubble CPAP in the NICU, standardizing the approach to weaning nasal CPAP, and adherence with the weaning guidelines (Fig. 3). Adherence with the nasal CPAP weaning guidelines was defined as the infant being weaned as per the weaning criteria of predetermined age and weight. The change concepts involved changing the workplace environment, managing the variations in practices, and designing the system to avoid mistakes. The subsequent interventions were implemented utilizing PDSA cycles.

Driver diagram for the bubble CPAP quality improvement project. NICU, neonatal ICU; RT, respiratory therapist; SMART, specific, measurable, attainable, realistic, and time-bound.
To manage the variation in the care provided to the infants within PDSA cycle 1, we introduced guidelines and weaning criteria of CPAP to create a standardized routine among all providers. The task force presented the guidelines to all faculty in the neonatal division meeting and communicated the information via e-mail. To positively change the work environment, we implemented bubble CPAP multidisciplinary rounds to create alliances and improve access to the guidelines and weaning criteria by educating nurses, RTs, and providers.
In PDSA cycle 2, multiple techniques were implemented to design a system that could avoid mistakes. We used reminders by including information in the weekly update e-mails and having CPAP weaning signs on all the devices. We also collaborated with teams to avoid simultaneous weaning of the incubator and CPAP.
In PDSA cycle 3, we continued to use weekly reminders to providers while additionally incorporating changes to promote pre-feeding skills. We collaborated with other teams to encourage positive oral stimulation with human milk for infants while on CPAP. We ensured that there were 24 h between the infant being off CPAP and weaning from isolette. Additionally, it aimed to improve headgear adherence and trialed the Tortle headgear (Tortle, Louviers, Colorado).
In PDSA cycle 4, we continued to use weekly reminders and aimed to improve headgear adherence. We also implemented pre-feeding skills in infants greater than 34 weeks on CPAP and aimed to improve prong size adherence. We also included encouraging infants to be seen by speech therapy by 33 weeks, and we incorporated real-time/weekly feedback to the providers.
Outcome measures
The primary outcome was the rate of successful nasal CPAP wean at the first attempt. The process measure was adherence with CPAP weaning guidelines. Balance measures included the total number of days on respiratory support (including all support from the high-flow nasal cannula [HFNC] and above, including CPAP support), the total number of days receiving nasal CPAP, and the use of home oxygen. Other outcomes compared were the total days to full oral feeds, infants discharged on gavage feeding, and the total length of stay in the hospital.
The clinical and demographic variables compared between the 2 epochs in the study included GA, birthweight, sex, ethnicity, and inborn status. We also compared antenatal factors such as the use of steroids, chorioamnionitis (maternal fever > 38°C and use of antibiotics), and intrauterine growth restriction (< 10th percentile for weight). Postnatal factors included intubation, use of surfactant, use of caffeine, presence of patent ductus arteriosus (diagnosed by echocardiogram), the presence of intraventricular hemorrhage (diagnosed by ultrasound), and the incidence of BPD (diagnosed based on the respiratory support at 36 weeks postmenstrual age as per the National Institute of Child Health and Human Development. 16 Grade 2 BPD included infants on respiratory support of HFNC, nasal CPAP, or noninvasive ventilation, and grade 3 BPD included infants on invasive ventilatory support. The presence of sepsis, anemia, and gastroesophageal reflux was included from ICD-10 codes from the subjects’ charts.
Statistical analysis
Pre- and post-intervention groups were compared. Continuous variables were analyzed using the Student t test, and the categorical variables were analyzed using the chi-square test or Fisher exact test. Mann-Whitney U test was used for non-parametric analysis. Clinical characteristics of infants were presented as mean ± SD for continuous, normally distributed variables; as median interquartile range (IQR) for continuous, non-normally distributed variables; and as numbers with percentages for categorical variables. All analyses were done with SAS statistics version 9.4 (SAS Institute, Cary, North Carolina). Control and run charts were plotted using Microsoft Excel 2019 (Microsoft, Redmond, Washington). P values < .05 were noted as a significant difference between the 2 epochs. Post hoc analysis showed that a sample size of 95 for epoch 1 and 100 for epoch 2 was predicted to have a power > 95%, with alpha 0.05 for the primary outcome measure of successful wean off nasal CPAP in the first attempt. The Pennsylvania State University Institutional Review Board reviewed this project, and it provided an exemption as it was a quality improvement initiative.
Results
Of the 223 infants admitted to the NICU who were eligible between January 2018–December 2020, 195 infants were included in the study (Fig. 1). The other infants were excluded as transferred to an outside facility during the hospital stay; need for tracheostomy; congenital cardiac abnormality; and other complications such as neurologic abnormality, congenital malformation, re-intubation for surgery, and death. The clinical and demographic characteristics did not differ between the 2 epochs (Table 1). The 2 epochs included infants at a median GA of 29 weeks versus 30 weeks (epoch 1 with median GA 29 [IQR 28–31] weeks vs epoch 2 with median GA 30 [IQR 28–31] weeks, P = .47). The median birthweight of epoch 1 was 1,190 [IQR 940–1,490] g compared to epoch 2 with a median birthweight of 1,130 [IQR 960–1435] g, P = .73 and did not differ significantly. Among the 2 epochs, the incidence of BPD did not differ significantly (17% vs 16%, P = .87).
Clinical and demographic characteristics of the epochs
Data are presented as median (interquartile range) or n (%).
GA, gestational age; INSURE, intubation, surfactant, rapid extubation; BPD, bronchopulmonary dysplasia; IVH, intraventricular hemorrhage; PDA, patent ductus arteriosus; GERD, gastroesophageal reflux disease.
After the implementation of the bubble CPAP weaning guidelines, the adherence to the weaning guidelines improved from ∼60% to ∼80% (Fig. 4). The mean percentage of infants weaning successfully off CPAP to room air on the first attempt improved from 9.5% to 54% (P < .001) after the implementation of the CPAP weaning guidelines, as noted by the control chart in Figure 5.

Run chart of adherence with bubble CPAP weaning guidelines. Black horizontal lines indicate medians. PDSA, Plan-Do-Study-Act.

Control chart of infants with successful weaning off CPAP in the first attempt. Center line denotes the mean, with gray lines showing upper and lower control limits, respectively. PDSA, Plan-Do-Study-Act.
Comparison of respiratory outcomes in the 2 epochs
The total days of infants utilizing nasal CPAP support increased in epoch 2 compared to epoch 1 (25 median d vs 8 median d, P < .001). Other respiratory outcomes, such as the total days on respiratory support (25 median d vs 28.5 median d, P = .26) and the rate of infants discharged on home oxygen (16% vs 25%, P = .11), did not differ significantly between the 2 epochs (Table 2).
Infant outcome measures
Data are presented as median (interquartile range) or n (%).
*Any respiratory support ≥ high-flow nasal cannula.
Other secondary outcomes, such as total days to full oral feeds, were significantly reduced in epoch 2 compared to epoch 1 (22 median d vs 29 median d, P < .001). However, the rate of infants discharged on gavage feeding was 17% (P = .98) in both epochs. Furthermore, the total length of stay (52 median d vs 60 median d, P = .10) also did not differ between the 2 epochs. There were no reported nasal CPAP weaning–associated adverse events, such as nasal skin injury and trauma, in both epochs. There were no reintubations or escalation of care within 7 d of stopping CPAP.
Discussion
We performed a retrospective cohort study to determine the effects of nasal CPAP weaning guidelines with the gradual pressure weaning method in preterm infants under 32 weeks gestation. We found that more preterm infants were successfully weaned off nasal CPAP during the first attempt after the implementation of the predetermined weaning guidelines in the NICU. We also noted that the total duration of nasal CPAP increased, and the total duration needed to achieve full oral feeds was reduced after the implementation of the weaning guidelines. There were no differences in the total duration of any respiratory support, the use of home oxygen, the need for home gavage feeding, and the total hospital length of stay between the 2 epochs. These findings suggest that predetermined nasal CPAP weaning practices may be associated with greater success of weaning from nasal CPAP. The results of our study are consistent with prior studies that have shown an improvement in successful weaning off nasal CPAP with the use of predetermined weaning criteria and gradual pressure weaning of nasal CPAP in preterm infants. 14,15,17–19 A quality improvement study by Matlock et al 20 also noted that the implementation of a weaning protocol for noninvasive respiratory support improved outcomes.
Among the prior studies, the largest multi-center randomized controlled trial (RCT) by Jensen et al 16 noted that only infants born < 28 weeks gestation were successfully weaned from nasal CPAP during the first attempt with a gradual pressure wean. Nevertheless, our findings differed from Jensen et al 16 multi-center trial, but the result was similar to another single-center RCT. The reason for this discrepancy in successful wean during the first attempt is likely due to the modified stability and failure criteria used from the RCT by Amatya et al. 15 Our gradual weaning method was modified from Jensen et al 18 and included a decrease in CPAP to 4 cm H2O for 24 h prior to the removal of nasal CPAP. This practice allowed the clinical providers to discontinue nasal CPAP only if the infant demonstrated that the reduction in nasal CPAP pressure was tolerated. We observed that implementing weaning guidelines resulted in a significant improvement in the success rate of CPAP weaning on the first attempt. This highlights the importance of following proper weaning protocols, as ad hoc weaning may lead to unsuccessful CPAP weaning. This, in turn, can cause clinical concerns such as atelectasis, desaturations, and intermittent hypoxic episodes. It’s important to note that while the impact of these events may not be immediately noticeable during the NICU stay they may have long-term effects.
Prior studies 18,21 have not shown any difference in nasal CPAP duration. This differs from our results. However, we reported the total duration spent in nasal CPAP during the hospital stay rather than the nasal CPAP duration after the initiation of weaning. The increase in the total duration of nasal CPAP in our study is likely due to the nasal CPAP weaning practice that included a postmenstrual age of 32 weeks and a weight of 1,600 g or more at the time of wean. The increase in the total nasal CPAP duration but not in the total duration of respiratory support and reduction in the use of other respiratory devices in the second epoch may also infer that nasal CPAP was used as a primary mode of ventilation in this group rather than other modes of ventilation. Furthermore, the trial by Jensen et al 18 had no specific age and weight requirement for weaning. However, the median age at randomization was mentioned as 32 weeks, similar to our predetermined age criteria. Our study was unique from other studies as we utilized well-defined and stringent nasal CPAP weaning criteria of postmenstrual age 32 weeks and 1,600 g. The exception was made at 34 weeks postmenstrual age with no specific weight requirement. The predetermined postmenstrual age and weight have yet to be used by any prior studies to our knowledge. The age and weight criteria were based on past studies, 11,15,18 which noted that infants were more successful around 32–34 weeks postmenstrual age and beyond a weight of 1,600 g. The predetermined age and weight criteria may have prevented premature weaning of nasal CPAP and further trauma due to atelectasis and could promote healthy lung growth.
Our study also evaluated the relationship between feeding practices and the nasal CPAP weaning approach. We found that the duration of achieving full oral feeding by the infant improved after the implementation of the nasal CPAP gradual weaning method. This result may show an association between improved developmental skills and nasal CPAP wean at a predetermined age and weight in the preterm infants in our study. Prior studies have not established this outcome, whereas one study evaluated the time to reach enteral feed when comparing the use of CPAP with another respiratory device. 22 There was an initial concern about whether the expected increase in nasal CPAP duration during epoch 2 could lead to a delay in achieving full oral feeds. However, our study found that there was actually an improvement in the duration of achieving full oral feeds. Although this association has not been established, we speculate that as the nasal CPAP weaning guidelines resulted in a successful wean on the first attempt this allowed caregivers to focus on oral feeding and promoted improved feeding skills in preterm infants, unlike in epoch 1, where ad hoc weaning resulted in unsuccessful attempts to wean and may have resulted in a delay in achieving full oral feeds. Our study did not show a difference in the incidence of BPD, the total length of stay, or infants discharged on supplemental oxygen or gavage feeding, which is similar to prior studies.
Limitations
It is important to note that our study results are limited as the study was conducted retrospectively at a single center. Another limitation is that we utilized nasal CPAP with the nasal interface in epoch 1 versus bubble CPAP system with its FlexiTrunk nasal interface used in the epoch 2. Therefore, the study findings may have been influenced by the different devices and nasal interfaces used. We also acknowledge that the study’s limitations include not taking into account the duration of oxygen requirement after CPAP wean. We recognize that this information could have been valuable in determining whether a successful wean off CPAP would have reduced the total days of oxygen use, although we did not observe a significant difference in the use of home oxygen between the 2 epochs.
Conclusions
Our study found that following CPAP weaning guidelines based on predetermined age and weight criteria, along with the gradual weaning method, increased the success rate of weaning preterm infants off nasal CPAP during the first attempt in the NICU. Additionally, these infants achieved full oral feeds in a shorter period of time after the implementation of the weaning guidelines. These findings suggest that using predetermined nasal CPAP weaning practices may be beneficial to preterm infant care.
Footnotes
Authors' Contributions
Ms Mattikalli presented a version of this paper at the Eastern Society for Pediatric Research, held March 2022, Philadelphia, Pennsylvania; at the Pediatric Academic Society, held April 2022, Denver, Colorado; at the American Thoracic Society, held May 2022, San Francisco, California; at the Eastern Society for Pediatric Research, held March 2023, Philadelphia, Pennsylvania; at the American Thoracic Society, held May 2023, Washinton DC; and at the Penn State Pediatric Research Day, held October 2023.
Author Disclosure Statement
The authors have disclosed no conflicts of interest.