
Abstract
Introduction
The aim of this research study was to explore the smoking behavior of adult African male immigrant smokers living in Glasgow to inform and contribute to primary health promotion frameworks.
Methods
25 adult African male immigrant smokers living in Glasgow were recruited via consecutive sampling by soliciting for participation through the use of flyers, posters and word of mouth. Data collection occurred via semi-structured face-to-face interviews. The interviews were audio taped, after which verbatim transcription was carried out and the data analyzed thematically.
Results
The participants' smoking habits were influenced by cold weather environment as well as societal norms that appear to make the smoking habit more acceptable in Glasgow than Africa. It appears the more educated the participants were, the fewer cigarettes they smoked. However, there was only a slight difference in the number of cigarettes smoked between participants with a degree and those with a postgraduate degree.
Conclusion
The participants' smoking habits in Glasgow appear to have increased because of environmental variables associated with living in Glasgow, specifically the cold weather environment and high acceptability of smoking habits in Glasgow.
Introduction
Tobacco use is the leading cause of premature mortality and the second-leading cause of death in developed countries,1–4 accounting for almost 20% of all mortality. 5 From a public health perspective, persuading people to avoid taking up or to stop smoking is important in order to contribute to population-based health improvements. However, little is known about smoking behaviors within particular subgroups of populations, specifically those drawn from multicultural origins. This has highlighted from a public health perspective, the need for this study to contribute to the knowledge base on smoking behavior, focusing specifically on adult African male immigrants currently living in Glasgow. The Africans are a growing subgroup among immigrants to Scotland. The total population of Africans living in Scotland in 2004 was 5118, which amounts to 0.10% of the entire Scottish population. 6 The population of the African subgroup in Scotland increased to 19,700 between July 2011 and June 2012, which amounts to 0.4% of the Scottish population. 7 The Black and Minority Ethnic (BME) groups generally have worse health than the overall population in Scotland. 8
Whilst the picture concerning African smokers in the UK is known, 9 against the backdrop of the Glasgow profile, the habits concerning this subgroup remain unknown, consequently adding weight to undertaking this study. The study was limited to African male immigrants because African females are less likely to smoke. 10 It is important for those working within the public health sector to take into account factors that influence adult African male immigrants living in Glasgow to smoke. This will help to develop a proactive framework that will contribute to reducing the smoking rates among African male immigrants living in Glasgow. The aim of this research study was to explore the smoking behavior of adult African male immigrant smokers living in Glasgow to inform and contribute to primary health promotion frameworks. The objectives of the study were to describe factors that motivate African male immigrants in Glasgow to smoke; and to describe the awareness of harmful effects of cigarette smoking among the study group. The study also sought to describe whether the awareness of harmful effects of cigarette smoking affected the decision of study participants to smoke or not; and to describe the views of adult African male immigrant smokers living in Glasgow concerning accessing smoking cessation programs.
Methods
Qualitative methodology is a research approach used extensively by social researchers studying human behavior and habits.11–13 It follows an inductive, interactive, flexible and reflexive research process.11,14 In addition, it entails the collection and analysis of non-numerical data to search for patterns, themes and overall features.14,15
The qualitative research involved 25 participants, but contact with the participants lasted a lot longer.11,14,16 One-to-one interviews with each participant lasted 30–60 minutes. In qualitative research, interviews are designed with open-ended questions to allow maximum flexibility and freedom, and the research questions are modified sometimes depending on what is needed to draw out a detailed response.11,14,17 In this study, moreover, the sequencing and approaches to key questions were changed depending on the details that needed to be drawn out. The research study involved face-to face encounters with the participants in accordance with the demands of qualitative research.11,13,18
Consecutive sampling was considered for the study because it permits all of the participants from an accessible population who met the eligibility criteria over a specific time interval or a specific sample size to be recruited. 19 Selection of participants was achieved by soliciting through the use of flyers, posters and word of mouth during various African communities' meetings in Glasgow. The inclusion criteria for participants reflected certain characteristics. The participants were Africans (those that participated in the study appear to come from Sub-Saharan Africa), smokers, English speaking men between the ages of 18–60 and residing in Glasgow. Exclusion criteria included: non-Africans, African non-smokers, African male immigrants outside the age bracket (18–60), women, and those of African heritage but native to Scotland.
The interviews were recorded on audio tape with the permission of the participants. Face-to-face interviews were employed for this study because participants were comfortable with answering questions associated with smoking, since in their demographic it is widely considered an expected behavior in homes, social environments and even in school. 20
Results
The characteristics of the study sample, such as number of participants, age, number of cigarettes smoked, countries of origin and educational level, are represented in Figure 1. The effects of educational qualifications on smoking behavior of participants are represented in Figure 2. The determinants of smoking habits of the participants are tabulated in Figure 3 and represented in Figure 4. The participants were asked about the factors that motivated their smoking habits. In responding to the questions, four themes emerged. The themes were adventurous motivation, psychological motivation, cold weather environment and societal norms as determinants of smoking behavior. In addition, the views, perceptions and understanding of the participants on health risks associated with smoking habits were explored and their knowledge appears to be average. Furthermore, the participants' views about accessing smoking cessation programs were explored and many of them considered it irrelevant or a waste of time.
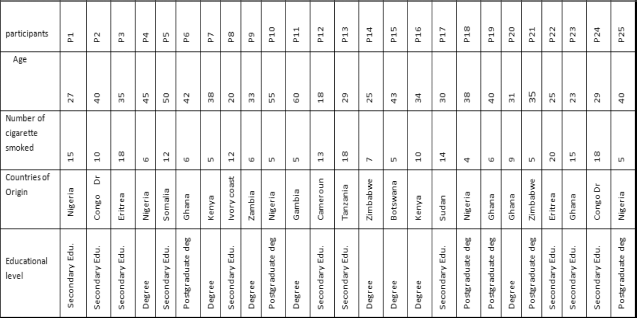
Characteristics of study sample.

Effects of educational qualification on smoking habits.

Determinants of smoking habits.

Representation of determinants of smoking habits.
The average number of cigarettes smoked per day by participants with secondary education is 15.3, whist participants with degree and postgraduate education smoked an average of 6.8 and 5.8 cigarettes respectively. There is a wide gap in the number of cigarettes smoked between participants with secondary education and those with degree education and above. It appears the more educated the participant, the fewer cigarettes they smoked. However, there is only a slight difference in the number of cigarettes smoked between participants with a degree versus those with a postgraduate degree.
Six of the participants (24%) were motivated to smoke by adventurous motivations–-to know what it feels like to smoke. A motivating factor for 10 (40%) of participants was psychological reasons such as anger, tension, stress, boredom and depression. Smoking in order to cope with the cold weather environment in Glasgow appears to motivate 8 (32%) of the participants. This was a unique finding, as smoking in order to cope with cold weather environments has not been discussed in the literature. Finally, the number of the participants that smoked because of their perception of smoking behavior as the societal norm in Glasgow is 14 (56%).
Health Risk Awareness
The views, perceptions and understanding of the participants on health risks associated with smoking habits are demonstrated below.
“It causes lung cancer.” P1:40
“It causes cancer of the lung, discoloration of the lung and skin.” P2:48
“I actually know what it does… I know the lung, the heart diseases it causes. I also know that it reduces your life span. Smoking is dangerous to health.” P4:31
“I know that cigarette smoking is not good to asthmatic patient because it can choke them.” P4:43
“It leads to shorter life span. Smokers are liable to die young.” P5:47
“Cigarette smoking is detrimental to health. I know that it has effect on pregnant women. It makes their babies to lose weight.” P7:39
Moreover, the smoking behavior of the participants may be linked to the assumption that an individual can be vulnerable only when involved in heavy smoking. This perception is demonstrated by the views of participants expressed below.
“[I]am not easily addicted to anything.” P10:49
“It causes lung cancer but depends on how you take care of yourself… the number you smoke.” P12:33
“I found that some people nicotine does not have an effect on their blood system using myself as an example.” P14:51
“After all, somebody lived hundred and something years and he was a smoker.” P18:52
“‘By level of my training I know that it is bad to smoke but I still do it.” P20:47
“Although I know smoking is harmful… that does not mean I must suffer from cancer.” P21:28
Participants’ Views concerning Accessing Smoking Cessation Programs
Accessing smoking cessation programs was considered by the respondents as irrelevant and a waste of time. Some of their views are presented below.
“I don't think smoking cessation group will help if you don't have the will to stop.” P1:55
“If I wish to stop, I can stop on my own will. Joining a smoking group is not relevant since I can control myself.” P1:58
“It is a waste of time, if I decide I can stop on my own.” P2:60
“Yes the addictiveness is there according to research; to me I feel that it is all about a person, if I want to stop I stop.” P3:63
“There is conviction in me that I do not need this therapy to stop.” P3:68
“When I used one, it affected my heart palpitation. My heart was beating quickly. I didn't like it.” P5:50
“Using patches, Nicorette gum and all that will help to stop smoking for a while but when they are not there, the smoker can go back to it.” P9:67
“What if you end up addicted to the products … and you don't have access to them, you may go back to smoking.” P10:70
Discussion
In exploring factors that motivate young and middle aged African male immigrants living in Glasgow to smoke, four themes emerged.
Adventurous Motivation
Most of the participants expressed that the inquisitiveness to experiment with smoking started at a very young age, especially during teenage years, and that they were motivated by the desire to know how it feels to smoke. Smoking for adventure has not been discussed in the literature. However, evidence in the literature on determinants of smoking behavior among teenagers in East Java province, Indonesia, reveals that the perception of adolescents that smoking is an adult behavior is one of the powerful motivators for the young people to smoke, in order to appear or feel older and mature. 21
Most of the participants stated that the moment initial smoking experimentation was undertaken, stronger affinity for smoking evolved fuelled by satisfaction and pleasure derived from it. This observation is in accordance with what was described in the literature, 22 which shows that smoking is a pleasurable act for young people in Canada. Moreover, the strong affinity for smoking was taken to the next level as the respondents reported inseparable smoking habits with some daily activities. This finding is in line with the Health Belief Model (HBM) principle of perceived benefits, which suggests that an individual (eg, smokers) will not perform an action (eg, smoking) if he/she does not think that doing so will improve his/her life. Examples in this study included perceived assistance of cigarette smoking in digestion of food. Some participants also said they smoked in order to develop courage and boldness to support communicating with the opposite sex.
Psychological Motivation
All the participants noted that psychological variables such as stress, worry, anger, depression, boredom and tension influenced their smoking behavior. This finding concurs with the evidence widely reported in the literature.23–28 By extrapolation, most participants believe that smoking takes away stress. This finding is in accordance with the principle of perceived benefits, in that smokers retain the action of smoking because they think it will improve their lives by reducing stress. Hence, smokers feel the need to smoke in order to reduce stress associated with daily life activities.
Another principle of the HBM suggests that the probability of an individual (eg, a smoker) changing his/her action (eg, smoking behavior) to avoid a consequence depends on how serious the person considers the consequences of his action (smoking) to be. Most participants attached more value to perceived benefits of smoking than the perceived severity of the consequences of smoking. With respect to this principle, it is clear that most participants enjoy the benefit of stress reduction offered by smoking and ignore its harmful effect.
Cold Weather as Determinants of Smoking behavior
Most interestingly, some participants explained that their smoking habits whilst residing in Glasgow had been enhanced because of the experiences of dealing with cold weather. This appears to stimulate an increase in their smoking behavior compared with dealing with hot weather in Africa, which tends to discourage smoking habits. This appears as a unique finding as there is little if any reference in the literature to the influence of cold weather in stimulating smoking habits. The reason the participants are motivated to smoke more in Glasgow than Africa appears to be the perceived benefit that smoking helps to heat up the body systems. By extrapolation, this practice of smoking may be a result of the need to adapt to the new experience of cold weather, which is unfamiliar to these participants as African weather is usually hot.
On the contrary, the reason participants tend to smoke less whilst residing in Africa reflects the Theory of Planned Behavior, which suggests that if an individual perceives that the outcome from performing a behavior is negative, the person will have a negative attitude towards performing that behavior. 29 In this instance, the participants perceived smoking under the hot sun in Africa as negative behavior. Hence, the respondents expressed negative attitudes towards performing the smoking behavior in that setting.
However, there are some studies that would appear to contradict this finding. For example, an evaluation study conducted in New Jersey for the period of 1999–2006 found that February, a winter month in the USA, had lower sales and lowest cigarette consumption compared with the summer month of June. 30 This finding concurs with what is demonstrated in the literature.31–33
The variations between this unique finding and previous findings may be as a result of the fact that the month of February has fewer days for distributors to purchase tobacco. In addition, it may be as a result of cigarette excise tax increase during that period. Tax increases have been shown to minimize smoking habits.34,35 Noteworthy is that New Jersey increased the state cigarette excise tax three consecutive times during the course of the aforementioned study, at the beginning of the fiscal year in 2003, 2004 and 2005.
Societal Norms as Determinant of Smoking behavior
Most of the participants stated that the rates of their smoking habits increase in Glasgow because it is considered a societal norm. In fact, most of the respondents believe that everybody in Glasgow smokes, especially the Scots. This perception encourages the participants to smoke frequently in order to be culturally accepted and fit in. This phenomenon agrees with the concept of social cognitive theory that identifies human behavior as interaction of personal factors and the environment.
This implies that the enhanced affinity for smoking expressed by the participants is a resultant effect of personal (participants') interaction with their social environment (where everybody is perceived to be a smoker). However, a report by the Lothian NHS Board seems to contradict the perception of the participants that everybody in Glasgow smokes. 36 The report findings state that the smoking prevalence of individuals aged from 16 and over in Glasgow ranges from 27.4% in Glasgow Kelvin (25.3% female, 29.7% male) to 40.1% in Glasgow Shettleston (38.3% female, 42.0% male). This finding is corroborated by a report from NHS Scotland. 37
According to the participants, the fact that the social norms in Glasgow do not frown at smoking behavior make it more acceptable, unlike the African norm, which frowns at smoking habits. Most of the participants argued that African culture does not encourage smoking behavior but instead discourages it. The participants reasoned that it is a mark of disrespect to smoke in front of their parent. Moreover, participants stated that social norms in Africa consider smoking as an act of way wardness and irresponsibility.
Health Risk Awareness
The participants demonstrated some level of awareness of the health implications of cigarette smoking. Specifically, most participants identified that cigarette smoking causes lung cancer, reduces life span and has effects on pregnant women. In addition, some participants also identified that smoking is dangerous to asthmatic patients and can also cause the discoloration of skin and lung. The level of health risk awareness demonstrated by the participants can be described as average. However, smoking has been linked with other diseases such as respiratory tract infections (eg, pneumonia and chronic bronchitis), emphysema (collapse of small airways in lungs), different kinds of cancer such as throat, mouth, kidney, bladder, pancreas, cervix and stomach cancer,38,39 as well as lung cancer, as identified by the participants. Smoking has also been implicated in leukemia, loss of bone mass and risk of fracture as well as cerebrovascular diseases, among many others.37,40
Critically analyzing the relationship between the level of health risk awareness among the participants and their smoking status, it is suggested that the level of health risk awareness could have been enough for the participants to abandon their smoking habits, but instead the participants continue to smoke. This practice of continuing to smoke irrespective of health risk awareness can be explained by the first principle of HBM, which states that individuals' willingness to change health behaviors is due to perceived susceptibility (eg, smokers will not change their health risk behavior unless they believe that they are at risk, such as the risk of lung cancer). In agreement with this principle, the participants may refuse to change their health risk behavior (smoking habits) and continue to smoke, probably because of the thinking that it does not make them vulnerable to diseases. Moreover, this may be linked to the assumption by the participants that an individual can be vulnerable only when involved in heavy smoking.
Participants’ Views concerning Accessing Smoking Cessation Programmes
Most of the participants expressed their ability to quit smoking without accessing smoking cessation programs. Accessing smoking cessation programs was considered by the respondents as irrelevant and a waste of time. This finding accords with a qualitative research study that employed focus group interviews as a means of data collection, which revealed that student smokers showed a lack of interest in accessing smoking cessation programs because they considered smoking cessation products such as nicotine replacement therapy, patches and Nicorette gum as a drug or chemical with side effects. 41
Correspondingly, some participants expressed absolute displeasure after experimenting with smoking cessation products. Some participants argued that smoking cessation products are ineffective. Their line of reasoning suggested that if an individual employs smoking cessation products to aid quit attempts, when the products are not available the person will revert to smoking. The finding of this belief is in accord with what is described in the literature. 42 Furthermore, some participants argued that they are not nicotine dependent. Hence, they stated they had no need for accessing smoking cessation programs as a result of their ability to quit unaided.
Implications of the Findings to Public Health Practice
The inabilities of some participants that have made an effort to quit but were unsuccessful suggests that the participants may be addicted to smoking. In view of this, health education on the signs and symptoms of cigarette addiction should be helpful to enlighten the African male immigrant smokers in Glasgow, via community meetings to help them make informed choices on quitting smoking. Health education is necessary since participants believe that only when an individual is addicted to smoking can the person be vulnerable to associated health risks.
The proposed health education should also involve reasons to avoid smoking, such as the addictive nature of cigarettes, difficulty of quitting and dangers of passive smoke to non-smokers. The health education may be organized by public health practitioners, smoking cessation specialists and/or other health protection professionals, in the form of seminars and workshops, and be implemented in African community meetings. To this end, local partnerships should be encouraged to bring local agencies, professionals and a wide range of approaches, professionalisms, perspectives and resources to bear on local problems. 43
In addition, there is a need to address the determinants of smoking through health education while observing ethnic, cultural and social differences associated with smoking. This suggestion is informed by the emergence of a unique variable (cold weather) which appears to play a role in smoking behavior among African male immigrants living in Glasgow.
Consequently, the smoking cessation intervention strategies should be comprehensive and their development should involve the knowledge of environmental factors as determinants of smoking behavior. To this effect, a new smoking cessation framework that incorporates the new determinant of smoking habits should be specifically and specially designed for African male immigrant smokers. For example, a smoking cessation framework that enables public health practitioners to motivate African male immigrant smokers to employ positive health attitudes such as drinking hot tea or coffee, the use of a gym, cycling or other sporting activities to overcome the influence of cold weather, which stimulates their smoking habits, may be helpful in tackling the health risk.
It is also important to strengthen the African culture, norms and value systems that discourage health risk behavior such as smoking. This practice could be achieved by establishing a working partnership between the public health sector and African parents and organizations on the need to inculcate African values that discourage health risk habits in their children. This practice will also enable the younger African generation to decline taking up the harmful habit. Interdisciplinary collaborations need to be widened to involve other role models, such as teachers and peers. The involvement of parents, teachers and peers in emphasizing the reasons that people should not smoke, to counteract the perceived reasons for smoking, should be helpful in dissuading individuals from smoking.
Moreover, most of the participants demonstrated that their smoking behavior stems from desire to reduce stress associated with daily life. In relation to this, it is necessary that African male immigrant smokers living in Glasgow are educated on the need to use conventional methods, such as listening to music, playing the piano, watching movies or playing with a pet, to minimize stress, instead of tobacco use, since it has harmful effect on the body over time. In other words, African male immigrant smokers should be informed that the perceived benefit in the smoking habit with respect to stress reduction is less than the potential harm associated with smoking behavior.
In addition, increasing the price of cigarettes may affect the number of cigarettes that African male immigrant smokers consume per day, since most participants stated that their smoking habits are influenced by its affordability.
Moreover, health promotion and smoking cessation messages can be transmitted through media such as newspaper articles, radio and television broadcast to reach the wider population of African male immigrants smokers in Glasgow. In addition, setting realistic goals for quitting and modeling sports, music and movie personalities who have quit successfully may encourage quitting attempts among African male immigrant smokers, since some of the participants expressed that such personalities that smoke influence their smoking behavior. Finally, pictorial representation of various disease conditions associated with smoking habits, such as emphysema and oat cell carcinoma, via public health workshops in African community meetings may be helpful in dissuading current smokers from continuing to smoke and prospective smokers from up taking the habit.
The limitation of this study was that the number of participants involved in the study was relatively small sample. Therefore, the study can only be generalized if the findings are confirmed in a quantitative study with larger study samples.
Conclusion
The participants' smoking habits in Glasgow appear to have been increased because of unique variables in Glasgow that influence their smoking behavior, such as its cold weather environment and the high acceptability of smoking habits in Glasgow. On the contrary, hot temperatures in Africa seem to discourage smoking. In addition, the smoking habit was perceived to be less acceptable in Africa. In light of these findings, it is necessary that community-based approaches to health be integrated into a range of government policy objectives. 44 This integration may occur at a local level, emphasizing collaborations between local communities (eg, African community organizations) and statutory agencies within the community. 44 Such government policy may include Standard Regeneration Budget, New Deal for Communities and the Neighbourhood Renewal Programme. 45 The aim should be to bridge the gap in health inequalities. This practice may provide opportunities to dissuade African male immigrants living in Glasgow from up taking the harmful smoking habit.
Recommendations for Further Research
Smoking for adventure has not been discussed in the literature. To this effect, it is necessary to employ a study that involves a larger sample to validate this finding or otherwise. Moreover, there is a gap in the literature on the influence of cold weather in stimulating smoking habits. To this end, a study that involves larger samples is needed to validate this finding or otherwise. Finally, there is a gap in the literature on the influence of African culture, norms and value systems on smoking behavior.
Author Contributions
Conceived and designed the study: EAE. Analyzed the data: EAE. Wrote the first draft of the manuscript: EAE. Made critical revisions: EAE. All authors reviewed and approved of the final manuscript.
Footnotes
Acknowledgement
The author is grateful to the participants for taking part in the studies.
As a requirement of publication the author has provided signed confirmation of compliance with ethical and legal obligations including but not limited to compliance with ICMJE authorship and competing interests guidelines, that the article is neither under consideration for publication nor published elsewhere, of their compliance with legal and ethical guidelines concerning human and animal research participants (if applicable), and that permission has been obtained for reproduction of any copyrighted material. This article was subject to blind, independent, expert peer review. The reviewers reported no competing interests.