
Abstract
Tobacco smoking remains the single most preventable cause of morbidity and mortality in developed countries and poses a significant threat across developing countries where tobacco use prevalence is increasing. Nicotine dependence is a chronic disease often requiring multiple attempts to quit; repeated interventions with pharmacotherapeutic aids have become more popular as part of cessation therapies. First-line medications of known efficacy in the general population include varenicline tartrate, bupropion hydrochloride, nicotine replacement therapy products, or a combination thereof. However, less is known about the use of these products in marginalized groups such as the indigenous, those with mental illnesses, youth, and pregnant or breastfeeding women. Despite the efficacy and safety of these first line pharmacotherapies, many smokers continue to relapse and alternative pharmacotherapies and cessation options are required. Thus, the aim of this review is to summarize the existing and developing pharmacotherapeutic and other options for smoking cessation, to identify gaps in current clinical practice, and to provide recommendations for future evaluations and research.
Keywords
Tobacco Use
Since the 1950s, we have observed significant reductions in tobacco use prevalence across many countries.1–4 Despite these reductions, tobacco smoking remains the single most preventable cause of morbidity and mortality, contributing to more drug-related hospitalizations and deaths than alcohol and illicit drug use combined. 1 Every year, approximately 5.4 million people die from tobacco-related diseases, translating to 1 in every 10 deaths among adults worldwide. 5 Tobacco use is known to cause up to 90% of all lung cancers and is a major risk factor of coronary heart disease, stroke, peripheral vascular disease, chronic obstructive pulmonary disease, reproductive and fetal developmental diseases, and many other conditions.1,6 Tobacco cessation, even after a short period of time, is known to produce significant health benefits within as little as 20 minutes. Within 12 weeks of smoking cessation, improvements in oxygen transportation, smell, taste, breathing, energy, and immune responses are observed. Within 12 months, the risk of coronary heart disease will return to half that of a current smoker and is reduced to that of a non-smoker by 15 years. 7 Moreover, smoking cessation treatments have greater cost effectiveness and clinical efficacy in comparison to other preventative health measures such as treatment of hypertension and hypercholesterolemia,8–10 and research has shown that the cost per life year saved by smoking cessation interventions makes it one of the most cost-effective health care interventions.10,11
For these reasons, assisting individuals to stop smoking is a key health improvement objective in many countries12–14 and pharmacotherapeutic options are increasingly being considered, particularly for individuals with high levels of nicotine addiction. Current first-line pharmacotherapies include nicotine replacement therapy, bupropion hydrochloride, and varenicline tartrate, with research suggesting that combining these with behavioral counseling increases efficacy and helps smokers achieve long term abstinence. 15 Yet, these medications show some limitations and significant resources are invested into the development of designer smoking cessation pharmacotherapies, which target specific pathophysiological mechanisms in nicotine addiction in an attempt to improve the effectiveness and safety of pharmacotherapeutic cessation aids. In addition, adaptation of medications used primarily to treat other conditions which have the potential to act as smoking cessation aids are also being evaluated, 16 as are novel adaptations to existing smoking cessation treatments.17–19 As such, this article is intended to provide the reader with an overview of current and emerging pharmacotherapeutic options for smoking cessation and provides recommendations for clinical practice, future evaluations, and research.
Current Pharmacotherapeutic Options for Smoking Cessation
The choice of any pharmacotherapy for smoking cessation should be guided by an individual's preference, contraindications, and precautions for use. 13 Consideration should be given to specific factors such as the potential for adverse events, possible drug interactions, the individual's experience with pharmacotherapy, convenience, availability, and cost before prescribing any pharmacological interventions to aid smoking cessation. 10 The level of nicotine addiction the individual is reported to have should also be taken into account based on a validated scale such as the Fagerström test for nicotine dependence. 20 Smoking cessation guidelines and treatment algorithms recommend the use of pharmacotherapy only in the presence of nicotine addiction to increase chances of a successful quit attempt, while non-pharmacological support is recommended for smokers who are not nicotine-dependent and those unwilling or unable to use pharmacotherapy.10,13,14,21 A systematic search of the Cochrane Database of Systematic Reviews’ Tobacco Addiction Group register was conducted to identify current and emerging pharmacotherapeutic options for smoking cessation. In addition, a search of Medline, EMBASE, and online clinical trial registries were also conducted with the key words smoking OR tobacco OR nicotine OR tobacco cessation OR smoking cessation AND pharmacotherap*. First-line pharmacotherapies have been listed in ranked order of efficacy.
First-Line therapies
Varenicline tartrate (Chantix or Champix) is a nicotinic receptor partial agonist designed to selectively activate the α4β2 nicotinic acetylcholine receptor. It blocks the effect of subsequent nicotine challenge on mesolimbic neuronal dopamine release, while mimicking the action of nicotine, causing the release of mesolimbic dopamine. 22 Clinical practice guidelines report that varenicline is the most effective form of single pharmacotherapy for smoking cessation based on available evidence. 10 A Cochrane meta-analysis of 14 trials comparing varenicline to placebo with respect to quit rate produced a risk ratio of 2.27 (95% CI 2.02 to 2.55), and compared to pharmacologically unassessed quit attempts varenicline improved the chances of long-term abstinence by two- to three-fold. 23 Statistically significant improvements have also been shown with varenicline for patients admitted to the hospital with smoking-related illnesses at 12 months follow-up. 24 Varenicline is reported to be a superior smoking cessation aid to date for long-term abstinence in the general population, with direct and indirect comparisons with bupropion, 100 nicotine replacement therapy products, 86 and cytisine. 101 The most common adverse event is nausea, which is reported to be mild, self-limiting, and resolving over time (RR 3.28; 95% CI 2.89 to 3.73). Further details pertaining to dosing and prescription, efficacy, and adverse events are reported in Table 1.
Comprehensive summary of first line therapy options for smoking cessation available at present.
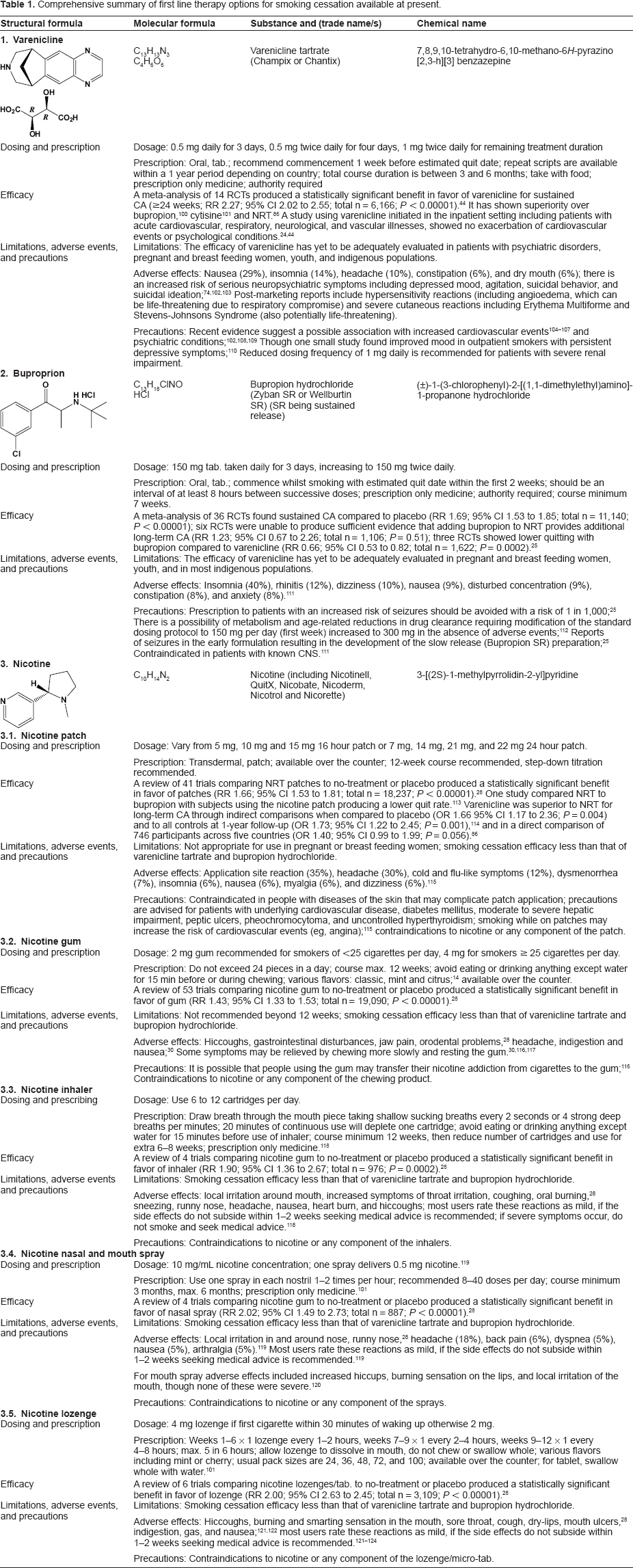
Bupropion hydrochloride (Zyban SR or Wellbutrin SR) is a norepinephrine and dopamine re-uptake inhibitor that decreases nicotine cravings and symptoms of withdrawal 26 while also interacting with neural pathways underlying nicotine addiction. 25 It can also be used as an antidepressant and is thought to reduce the depressive symptoms of nicotine withdrawal, as nicotine itself may cause antidepressant effects that bupropion helps maintain. 26 Evidence from clinical trials report that bupropion aids long-term smoking abstinence when compared to placebo and nicotine replacement therapy products; however, when compared to varenicline, it showed reduced quitting success.23,25,27 The most common adverse events include insomnia, dry mouth, and nausea. 25 Further details pertaining to dosing and prescription, efficacy, and adverse events are reported in Table 2.
Comprehensive summary of other pharmacotherapeutic options for smoking cessation available at present.

Nicotine replacement therapy (NRT) products are designed to control cravings by replacing nicotine through various delivery systems. Nicotine patches differ from other NRT products (eg, lozenges and gum) in that they deliver nicotine slowly and passively over time. 28 Transdermal patches are available in doses varying from 5 mg to 22 mg over a 16- to 24-hour period. Lozenges and chewing gum are available in strengths of 2 mg or 4 mg; however, no available NRT products deliver nicotine as quickly as a cigarette, being between 1 mg and 3 mg of nicotine per cigarette with the typical pack-per-day smoker absorbing 20 to 40 mg of nicotine per day.28,29 The most recent product on the market is the nicotine quick mist, which is a 1-mg oral mouth spray that produces levels of plasma nicotine similar to nicotine gums and lozenges. 30 A review of 132 trials found that NRT patches improved the likelihood of successful smoking cessation by 50% to 70% regardless of the setting. 28 NRT products are available over the counter and the major side effects vary depending on the type of product, but typically include skin irritation from patches and irritation to the inside of the mouth from gum and tablets. 28 Further details pertaining to dosing and prescription, efficacy, and adverse events are reported in Table 1.
Other Pharmacotherapeutic Treatment Options for Smoking Cessation Nicotine Receptor antagonists
Nicotine receptor antagonists include varenicline tartrate (as reported above), cytisine, dianicline, and mecamylamine, all of which moderate levels of dopamine to counteract withdrawal symptoms (agonist) and reduce smoking satisfaction (antagonist). 23 A detailed summary of varenicline is described above and cytisine shows the highest efficacy of the remaining nicotine receptor agonists. A review of nicotine agonists identified one trial examining dianicline as a smoking cessation therapy, which was found to be ineffective. 23 A separate Cochrane review examining mecamylamine identified two studies for inclusion, the results off which suggested that a combination of nicotine replacement therapy and mecamylamine may be superior to nicotine replacement therapy alone. 31 However, these results were based on two studies with small sample sizes, and confirmation in larger studies is required before the treatment can be recommended clinically. 31
Cytisine (Tabex) is derived from the plant Cytisus laburnum and acts as a low-efficacy partial nicotine agonist binding to subtypes of neuronal nicotine receptors, particularly the α4β2 subunits. Recent studies have highlighted the potential for this drug to be used in low- to medium-income countries27,33 where tobacco cessation is not supported by insurance plans or the national health service 23 as well as in the indigenous setting. 34 Efficacy trials show modest improvements in quit rates with outcomes similar to studies using nicotine replacement therapy, 23 though twice as effective as placebo. 34 Further details pertaining to dosing and prescription, efficacy, and adverse events are reported in Table 2.
Pharmacological therapies that are used primarily to treat other medical conditions may also be used for treating nicotine addiction. As research aimed at exploring and understanding the biological mechanisms of nicotine addiction develop, new opportunities are arising for existing pharmacological agents to be translated into the tobacco arena. The following section provides a summary of such medications, which have potential applications in treating nicotine addiction.
Anxiolytics
Anxiolytics are proposed as a smoking cessation treatment because of their ability to abate anxiety, one of the common symptoms of smoking cessation. 35 There are many types of anxiolytics that may have a role as smoking cessation treatments including clonidine, buspirone, diazepam, doxepin, meprobamate, ondansetron, and the beta-blockers metoprolol, oxprenolol, and propanolol. 35 The anxiolytic clonidine has the most evidence evaluating efficacy for smoking cessation out of the nine anxiolytics, and as such are a more detailed description of clonidine is reported below and in Table 2.
Clonidine is marketed as an antihypertensive but also has applications for drug and alcohol withdrawal symptoms,36,37 as a treatment for chronic pain, 38 menopausal flushes39,40 and Tourette's syndrome. In a systematic review of tobacco withdrawal symptom studies, clonidine has been reported to ameliorate cravings, anxiety, restlessness, tension, and hunger, but also caused some side effects such as sedation, dry mouth, and dizziness, with twice as many patients taking clonidine discontinuing medication compared to placebo. 42 For these reasons, clonidine is not considered a first-line treatment; however it may be beneficial for targeted populations such as smokers who are likely to experience high levels of anxiety and agitation when stopping smoking and subsequently may benefit from the sedative effects. 42 Further details pertaining to dosing and prescription, efficacy, and adverse events are reported in Table 2.
Other Antidepressants
Other antidepressants, including tricyclics (doxepin, imipramine, and nortriptyline), monoamine oxidase inhibitors (moclobemide and selegiline), selective serotonin reuptake inhibitors (fluoxetine, paroxetine, and sertraline), atypical antidepressants (bupropion–- mentioned above, tryptophan, and venlafaxine), and extracts (St. John's Wort–-Hypericum perforatum L.) have also been examined as smoking cessation aids. 25 A Cochrane review of antidepressants for smoking cessation identified 66 trials, 49 or which were investigating bupropion and 9 nortriptyline. 25 Pooling of bupropion and nortriptyline studies indicated long-term smoking cessation efficacy similar to that of nicotine replacement therapies, while selective serotonin reuptake inhibitors did not. 25 As bupropion is discussed above as a first-line smoking cessation aid, a detailed summary of nortriptyline is reported below and in Table 2 as it shows the most evidence of the remaining antidepressants for use as a smoking cessation medication.
Opioid Antagonists
Opioid antagonists including naltrexone, buprenorphine, and naloxone are thought to be potentially effective smoking cessation medications as they have the potential to attenuate the rewarding effects of cigarette smoking. 43 Smokers report both positive and negative effects associated with smoking with the reinforcing properties of nicotine theorized to be mediated through the release of various neurotransmitters in the brain. There is evidence to suggest that the endogenous opioid system may have a reinforcing role in smoking, while other studies report that the system may also have a mediating role with nicotine withdrawal. 43
Naltrexone is a long-acting opioid agonist marketed as a drug that blunts certain effects of narcotics such as heroin, meperidine, morphine, and ocycodone and is also used in the treatment of alcoholism. 43 Naltrexone is thought to reduce nicotine cravings by diminishing the activation of mesolimbic dopamine receptors; thus, combination therapy with NRT is thought to offer an additive effect for achieving smoking abstinence due to its different mechanisms of action. 43 Further details pertaining to dosing and prescription, efficacy, and adverse events are reported in Table 2.
Cannabinoid Type 1 Receptor antagonists
Cannabinoid type 1 receptor antagonists such as rimonabant and taranabant are thought to assist smoking cessation by restoring the balance of the endocannabinoid system, which can be disrupted with prolonged exposure to nicotine. Central cannabinoid receptors have been implicated in brain reward function and are thought to play a role in dependence and habituation. 44 It is thought that rimonabant may work by blocking the central cannabinoid receptors thus restoring the balance and inhibiting nicotine and food cravings. 44
Rimonabant was originally manufactured to treat obesity and was later proposed as a smoking cessation aid due to its potential for protecting successful quitters from significant post-cessation weight gain. Smoking cessation itself is associated with weight gain, which deters some smokers from making quit attempts; it was hoped that rimonabant would act as a cessation aid for these smokers. Reports of increased levels of suicidal thoughts and depression resulted in withdrawal of rimonabant as a prescription drug in European Countries in 2008. 44 Further details pertaining to dosing and prescription, efficacy, and adverse events are reported in Table 2.
Lobelia
Lobelia (lobeline) is derived from the Indian tobacco plant Lobelia inflate and was first synthesized in the early 1900s when it was classified as a partial nicotinic agonist. 45 The first documented use of lobeline as a smoking cessation treatment was in the 1930s with a variety of dosages and delivery mechanisms tested since then, including tablet (8 mg as lobeline sulphate), parenteral injection, buffered tablets, and flavored pastilles. 46 All of these formulations produced varying degrees of adverse effects including gastric side effects, dizziness, nausea, vomiting, and throat irritation.47,48 In 1993, the FDA announced a ban on all over the counter smoking cessation products in the United States due to a lack of efficacy data. 49 Further details pertaining to dosing and prescription, efficacy, and adverse events are reported in Table 2.
Silver Acetate
Silver acetate is designed to act as an aversive stimulus to inspire smoking cessation by producing an unpleasant metallic taste when combined with cigarettes. 50 Smokers are encouraged to use silver acetate products such as lozenges, gums, and sprays so that the act of smoking becomes unpleasant to diminish or stop the urge to smoke. 50 Efficacy studies have shown a possible small effect of silver acetate, though any benefit observed is less than that produced by nicotine replacement therapy (NRT) and therefore silver acetate is not widely used to promote smoking cessation in the clinical setting with the exception of a possible combination use with NRT. 50 Further details pertaining to dosing and prescription, efficacy, and adverse events are reported in Table 2.
Nicobrevin
Nicobrevin has been marketed as a smoking cessation aid in 11 countries including the United Kingdom (UK), New Zealand, and Germany, though in 2011 a governmental review found Nicobrevin to be ineffective as a smoking cessation aid and identified several side effects. Thus, the risks of the product outweighed the benefits. 51 This resulted in withdrawal of the product from the UK and other markets. Nicobrevin is a proprietary product containing four active ingredients, including quinine (15 mg, thought to reduce cravings), menthyl valerate (100 mg, acts as a sedative), camphor (10 mg, relieves respiratory congestion and gastrointestinal disturbances), and eucalyptus oil (10 mg, relieves respiratory congestion and gastrointestinal disturbances). 52 Further details regarding to dosing and prescription, efficacy, and adverse events are reported in Table 2.
Adaptive and Novel approaches
New formulations and innovative delivery systems for existing products are in development53,54 such as a straw containing nicotine beads, which allows the smoker to place drops of nicotine directly into a beverage, 19 though safety and efficacy data remains unknown. Galenic formulations of varenicline are also being developed, including a controlled release formulation (ClinicalTrials.gov Identifier: NCT00741884 and NCT005227150), a free base solution (NCT00774605), and a free base patch (NCT01234142, NCT01013454, NCT00774605). Tailoring dosages of existing medications such as varenicline and nicotine patches are also being evaluated with administration of up to 5 mg dosages per day of varenicline for smokers not experiencing any adverse events during the standard first week of titration (NCT01206010) and 42 mg patches for fast metabolizers of nicotine (NCT00956943). Combinations of existing products are also being explored as options for enhancing abstinence rates, with some evidence of success for combining varenicline with nicotine replacement therapy 55 (NCT01184664) and bupropion 56 (NCT00935818).
Electronic nicotine delivery systems or ‘E-cigarettes’ are becoming increasingly popular, particularly among the youth and adolescents as flavored varieties are now being introduced. 18 These small cigarette-shaped electronic devices use a battery-powered heating element, across which a solution of nicotine and propylene glycol (though other solutions are also used) is drawn. This causes the humectant to vaporize and subsequently be inhaled via a small tube as a mist. 17 Despite marketing of the product as a safe alternative to cigarette smoking as it does not contain the harmful ingredients normally found in cigarettes, there are concerns regarding the wide-spread use of these devices, with FDA reports of some tested samples containing toxic substances including nitrosamines and even diethylene glycol. 18 Moreover, many manufacturers still evade government regulation, raising issues around safety and harm reduction.17,18 E-cigarettes are currently being trialed for smoking cessation and reduction in smokers who are unwilling to quit (NCT01195597).
Immunotherapy, also referred to as nicotine vaccines, are currently being developed and evaluated through pharmaceutical studies some of which are phase III trials, with the most advanced vaccines expected to be launched in the first years of the 2010 decade.54,57 Nicotine is a small molecule that is unable to induce antibodies directed against it. 58 Immunotherapy is designed to chemically link nicotine to a carrier so that it acts as a hapten. 59 This allows antibodies to bind to nicotine molecules in the plasma, resulting in a nicotine-antibody complex too large to cross the blood-brain barrier. 60 Thus, anti-nicotine antibodies change the kinetics of nicotine accumulation in the brain as well as the distribution of nicotine between the brain and other body tissues. A review of four pharmaceutical trials found no long-term smoking cessation success to date, 61 with none of these studies reporting any major side effects (NCT01178346, NCT001102114, NCT01280968).
Alternative Medical Interventions and the Role of pharmacogenomics
To date, alternative therapies such as acupuncture, 62 hypnotherapy, 63 quit and win contests, 64 and exercise interventions 65 have, for the most part, been unsuccessful as a smoking cessation aid. There is evidence to support the use of behavior modification and cognitive interventions (including counseling and support programs), and these should be considered in combination with all pharmacological interventions24,66 and alternatives for people with contraindications to pharmacotherapies. 50
Studies are currently underway to test genetic factors that may predict the effectiveness of smoking cessation therapies, including varenicline (NCT01228175) and nicotine replacement therapy (NCT00326781). Additionally, examinations into potential genetic moderators of nicotine, such as the mu opioid receptor gene (OPRM1) A118G polymorphism, are being investigated with the hypothesis that AG/GG genotype smokers will have attenuated subjective-rewarding from intravenous administered nicotine compared to those with AA genotypes (NCT00969137). Specific nicotine biomarkers are also being evaluated to understand how these may influence a smoker's decision to quit (NCT01314001). Using biological indicators as a motivator for smoking cessation is not a new concept, with spirometric ‘lung age’ used as a persuader in the early to mid-1980s. 67 It is theorized that providing a smoker with an estimate of their individualized and personalized damage as a result of their tobacco use will motivate them into a quit attempt, though the exact mechanisms by which improvements are obtained remains unclear. 68
Specific Populations
Young People
Some evidence-based guidelines recommend nicotine replacement therapy as a means of cessation for youth aged 12 to 18 years who are dependent on nicotine (ie, it is not recommended for use by occasional smokers). 13 Other pharmacological interventions such as varenicline tartrate, however, have not yet specifically been evaluated for safety or efficacy in youth and should be considered with caution. Considering that tobacco use typically begins in childhood or early adolescence 69 with only 10% of new smokers initiating the habit after the age of 18 years, 70 more investigation is needed in this area, particularly to prevent youth from experimenting with tobacco use in the first place.
Gender Differences
Research suggests that gender differences exist in relation to nicotine dependence with females tending to smoke less and commence tobacco use at a later age than their male counterparts. 71 Females are also less likely to be tobacco-dependent and subsequently less responsive to nicotine replacement therapy and more responsive to the sensory and behavioral aspects of smoking, which should be considered when considering smoking cessation initiatives. 71 Moreover, clinical research trials suggest that females may be more susceptible to the effects of tobacco use with greater deterioration of lung function, and more severe disease in subjects with chronic obstructive pulmonary disease. 72
Hospitalized Individuals, Those Awaiting Surgery, and Cancer patients
Each medical institution should have their own system for assisting individuals with craving control during times of enforced abstinence such as hospitalization, where smokers may not be able to access outdoor areas to smoke. 13 This period of enforced abstinence also yields an opportunistic time to offer assistance to achieve long term abstinence. Varenicline tartrate has been trialed in hospitalized patients with tobacco-related illnesses, producing successful results at 12 months follow-up. 24 However, if craving control during hospitalization is the primary objective, then nicotine replacement therapy products offer the fastest delivery of nicotine to control cravings. 13 Additional cessation support should be offered to patients with multi-session treatments and medications continuing for at least one month post-discharge. 13 Smoking cessation pharmacotherapies for cancer patients are also recommended to assist with craving control during hospitalization or for obtaining long-term abstinence as described above. However, it is important to consider timing of quit attempts for these individuals due to physiological changes following cessation that may affect the metabolism of some drugs and targeting precision and accuracy of dose-volume histogram analyses for radiation therapy. 73
Individuals with Mental Health issues
Pharmacotherapies for smoking cessation have been specifically evaluated in individuals with mental health issues. There are contraindications for some products such as varenicline tartrate and bupropion hydrochloride, which carry boxed warnings from the FDA for people with suicidal ideation, self-injurious behavior, and severe depression. 74 People with mental health issues who stop smoking while taking medications for their illness should be monitored closely to determine if dosage reductions in their medications are necessary. 13
Pregnant and Breastfeeding women
It is well-known that smoking during pregnancy can have devastating health consequences not only on the mother, but also the unborn child including growth restriction, preterm delivery, and stillbirth.75–77 However, there are reports of up to 13% of women in the US 78 and 18% in France 79 continuing to smoke up until delivery, with higher prevalence estimates reported amongst indigenous women (45% during pregnancy increasing to 63% post-partum in one Australian population). 80 Nicotine replacement therapies can be considered for use by pregnant women; however, oral products are preferable to transdermal patches (for example gum, inhalers, micro tabs, and lozenges). 13 Potential adverse effects are associated with all smoking cessation pharmacotherapies; thus, psychological interventions should be considered as the first line of treatment during pregnancy. There is a lack of evidence regarding safety for the use of other forms of pharmacological smoking cessation therapies during pregnancy or while breastfeeding, though the risks of continued smoking must be weighed against the detrimental health consequences of continuing smoking.
Indigenous Populations
A 2012 Cochrane systematic analysis identified four studies evaluating pharmacological interventions for smoking cessation in indigenous populations globally. This review highlighted the paucity of data in this cohort, despite indigenous populations being over-represented in the burden of smoking related morbidity and mortality. 81 The authors were able to conclude that there was some evidence of effectiveness for combined pharmacological and cognitive initiatives that were culturally-tailored to the population; however, the evidence base is not strong and highlights the need for methodologically rigorous trials to bridge the gap between tobacco-related health disparities between the indigenous and non-indigenous populations. To date, FDA-approved nicotine transdermal patches and bupropion have been evaluated in the indigenous setting, producing some success in smoking abstinence, though studies are still needed to evaluate the safety and efficacy of varenicline tartrate.
Challenges to Consider
Although many believe that the tobacco epidemic is under control, the latest epidemiological evaluations in developing countries suggest otherwise, with an increase in youth tobacco use, particularly amongst girls aged 13–15 years; aggressive tobacco industry marketing campaigns are mostly to blame. 82 Moreover, the 2012 US Surgeon General's Report states that rates of decline for tobacco smoking amongst youth have now stalled with smokeless tobacco use once again on the rise (Centers for Disease Control and Prevention and US Department of Health and Human Services, 2012). For each person that dies because of a smoking related illness (more than 1,200 per day), at least two youths or young adults are becoming regular smokers. 2 This increase in youth tobacco use today means an increase in adult daily tobacco users tomorrow. As an example, had the success that was made between 1997 and 2003 been maintained in reducing youth tobacco use, there could potentially be three million fewer smokers in the United States of America today. 2 On a worldwide scale, tobacco use currently costs governments and consumers hundreds of billions of dollars each year in lost productivity and health care expenditures. 4 Data on the global impact of tobacco is incomplete; however, it is known to be high, with annual tobacco-related health care costs US$81 billion in the US, US$7 billion in Germany, and US$1 billion in Australia. 83 The cost in both human lives and economic resources will continue unless immediate action is taken to assist current tobacco users to quit, particularly those in high-risk populations, such as low- to medium-income countries, indigenous populations, and youth.
A major challenge for all tobacco researchers are smokers that are unwilling to quit. Most research to date has focused on highly motivated individuals who are eager to attempt cessation. However, recalcitrant smokers who continue to smoke despite the known consequences pose the greatest problems, yet attract the least amount of attention. This may partly explain why smoking cessation pharmacotherapies that succeed within a randomized controlled trial fail to completely translate into the real world setting. 15 Some research projects are underway to examine pharmacotherapeutic options for smokers unwilling to quit (NCT01195597); however, more research is needed. Similarly, insufficient research and clinical attention are given to maintaining abstinence once a person has made a quit attempt. Supporting long-term abstinence can be considered a costly endeavor over the short-term, requiring regular follow-up, prescription of ongoing pharmacological support, and alterations to existing cessation strategies that may require in-depth consultations and discussions with the individual regarding their quitting status. However, the long-term benefits such as improved health, reduced health care costs, lower governmental expenditure, and quality of life should outweigh the short-term output, but more research is needed in this area to encourage policy makers and governments to consider such initiatives. 84
Implications for Tobacco Cessation in Clinical Practice and Public Policy
Although many people will quit tobacco use unaided, for some, particularly those with greater nicotine addiction, pharmacotherapies may offer the extra support needed to produce a successful long-term quit attempt. Many comprehensive, evidence-based clinical practice guidelines for smoking cessation have been developed. These are regularly updated by local governments and health institutions10,12–14 and provide recommendations for clinical practice based on the latest available evidence. All of these guidelines recommend smoking cessation pharmacotherapies for smokers addicted to nicotine in addition to some form of regular counseling, as the chances of long-term abstinence are cumulative when used in combination. 12 Efficacy data to date suggest that varenicline tartrate offers the best chance of long-term successful quit attempts,44,86 while nicotine replacement therapy is ideally situated for short-term craving control and for individuals with contraindications to varenicline or bupropion. Advice from health professionals trained in smoking cessation strategies have been shown to increase the number and success of quit attempts among their patients. 87 Providing brief advice to most smokers (as little as 3 minutes) is more effective than spending longer time with a few patients. 10 Moreover, a Cochrane systematic review evaluating the training of health professionals in smoking cessation techniques found no evidence of additional benefits for interventions of greater duration over brief interventions. 87 It is important to remember that most patients will relapse multiple times before achieving successful long-term abstinence (known as the transtheoretical model of behavioral change theory), and guidelines for consultations are available to help individuals move from pre-contemplation to contemplation, preparation, action, and maintenance, which will eventually result in a successful quit attempt. 88
Recalcitrant and continued smoking fails to be classified in many medical circles as an illness, with too many health professionals considering tobacco use as an individual's right and freedom of expression foremost and as an illness second. Thus, implementation of tobacco cessation interventions is hindered. In reality, smokers become biologically dependent on nicotine, and until perceptions and attitudes within the health professions change, tobacco cessation programs will continue to be hampered.
Development of successful pharmacotherapies will do little if translation from research into public policy does not effectively occur. A multi-faceted approach is needed to increase the likelihood of success, which includes public policies such as smoking bans in public places, restrictions on the purchase of tobacco products, increased governmental legislations, and mass media awareness campaigns. Increased taxation of tobacco products has been shown to prompt smoking cessation attempts and reduce existing purchases of tobacco products, with research indicating that regular increases in tobacco tax may further encourage quitting activity. 89 Governmental policies including tobacco product content regulation with extreme de-nicotinization and smoke pH regulation of cigarettes by tobacco companies have the potential to significantly impact tobacco use by reducing the addictive properties within cigarettes. Such legislation is necessary and overdue in many countries, as absorption of nicotine across biological membranes largely depends on pH. 90 Thus, controlling the manufacture of cigarettes will reduce the addictive properties, allowing tobacco users to truly make an informed decision about wanting to smoke. As part of this multifaceted approach, smoking cessation training programs including motivational interviewing techniques for health professionals should be a mandatory component of medical training. Evidence confirms that a lack of training is a barrier to offering advice, as untrained health professionals report that they do not feel they have the skills, ability, or confidence to implement tobacco cessation programs,91,92 and yet the patients of health professionals trained in smoking cessation initiatives show statistically and clinically significant improvements in long-term abstinence. 87
Future Evaluations and Research(Gaps in Current Practice)
Nicotine addiction is a complex psychosocial, behavioral, and biological process that is not well-understood. For global reductions in tobacco use to occur, future researchers need to consider the biological and psychological aspects of nicotine addiction, as well as environmental factors contributing to existing levels of tobacco use prevalence. Particularly, a key area lacking investigation concerns the transportation of smokers from pre-contemplation through to action. Research is needed to identify motivational triggers among these individuals and determine existing barriers to smoking cessation. As technology advances, medical disciplines are moving toward the goal of personalized medicine, with individualized pharmacotherapies based on specific genetic and environmental factors associated with each individual smoker, which may increase the number of quit attempts. Researchers are consistently identifying new genetic properties that influence the pharmacokinetics and pharmacodynamics of nicotine, such as the polymorphism of the CYP2A6 isoenzyme, resulting in a developing field of research that requires attention. The inability of preliminary immunotherapy studies to produce efficacy in long-term smoking abstinence also requires investigation, with potential limitations of existing animal models under the spotlight. 57
Research into gender variances are needed to understand the impact that biological and cognitive differences have in smoking cessation strategies between the sexes, 71 particularly with evidence suggesting that females may be more susceptible to the lung-damaging effects of cigarette smoking than males. 72 Additionally, the steady increase in female tobacco use and reduction in male tobacco use over recent decades needs to be considered in relation to observed gender differences in addiction and health effects resulting from tobacco use. 93 Efficacy research examining existing pharmacotherapeutic aids for smoking cessation is also lacking in other specific populations such as youth, individuals with mental health issues, and indigenous populations.
There is a paucity of research to determine the efficacy of pharmacological interventions for smoking cessation in the indigenous setting, while most indigenous populations are overrepresented in the burden of substance-related morbidity and mortality. Current evidence suggests that significant amounts of resources are being invested, particularly by government bodies, yet methodologically rigorous evaluation procedures are significantly lacking. 81 This carries substantial dangers with funding being invested into ineffective programs (which is possible without effective evaluations to determine true treatment efficacy), resulting in an opportunity cost for potentially effective initiatives. 94 Moreover, the few previous studies report significant shortcomings relating to the effective implementation of research methodology as intended, particularly related to the uptake of pharmacotherapies and behavioral change interventions.81,94,95 This indicates that the next phase of tobacco-related research for the indigenous setting should be qualitative in nature to examine where and why difficulties in existing research projects have occurred and to determine how they can be overcome.
Qualitative research has been underutilized in the tobacco arena mostly due to concerns regarding methodological rigor and ambiguity in analyses resulting in qualitative analyses that lack strength. 96 However, because the nature of nicotine abuse is two-fold and includes physiological addiction to nicotine and behavioral components including habit, a mixed method approach (combination of qualitative and quantitative research) should be considered. This will facilitate more thorough evaluation of areas where existing evidence is lacking, particularly for the specific populations as listed above in which existing smoking cessation approaches produce little effect.81,97–99 Such process evaluations, particularly for key components such as context and fidelity, can provide essential information to intervention studies across all settings.
Conclusions
The most common pharmacological aids for smoking cessation include nicotine replacement therapy, varenicline tartrate, and bupropion hydrochloride, with varenicline producing the greatest chance of long-term abstinence. Clinical practice guidelines recommend the use of counseling programs in conjunction with pharmacological interventions, with regular follow-up and continued support to improve chances of success. Emerging pharmacotherapies include adaptations to existing treatments, evaluation of medications used to treat other conditions, and the use of genetic and biological factors that have the potential to influence the mechanisms of nicotine addiction. A primary objective of future research should be to develop initiatives, which may include high efficacy pharmacotherapies, to assist smokers who are not willing or report being unable to quit. Moreover, for smoking cessation pharmacotherapies to be successful, effective implementation strategies must be clearly established with a multi-faceted approach that includes instigation of public policies, tobacco taxes, adequate support structures, and easy access to low-cost medications with high treatment efficacy.
Author Contributions
Conceived and designed the manuscript: KC, MB, TR, RT. Analysed the data: KC, MB, TR, RT, AE. Wrote the first draft of the manuscript: KC. Contributed to the writing of the manuscript: KC, MB, TR, RT, AE, MP, BS. Agree with the manuscript results and conclusions: KC, MB, TR, RT, AE, MP, BS. Jointly developed the arguments and structure for the paper: KC, MB, TR, RT, AE, MP, BS. Made critical revisions and approved final version: KC, MB, TR, RT, AE, MP, BS. All authors reviewed and approved of the final manuscript.
Funding
Author(s) disclose no funding sources.
Competing Interests
Author(s) disclose no potential conflicts of interest.
Disclosures and Ethics
As a requirement of publication the authors have provided signed confirmation of their compliance with ethical and legal obligations including but not limited to compliance with ICMJE authorship and competing interests guidelines, that the article is neither under consideration for publication nor published elsewhere, of their compliance with legal and ethical guidelines concerning human and animal research participants (if applicable), and that permission has been obtained for reproduction of any copyrighted material. This article was subject to blind, independent, expert peer review. The reviewers reported no competing interests. Provenance: the authors were invited to submit this paper.