
Abstract
Objectives
This study evaluates the effects of a prison-based addiction intervention program. The evaluation is based on a multidimensional data collection that draws a portrait of the respondents’ substance use, and of their psychological/emotional, social, and judicial spheres. It measures the changes, or lack thereof, in substance use; the psychological/emotional, social, and judicial spheres; as well as the post-treatment services used.
Method
A quasi-experimental repeated measures design (0, 6 weeks, and 6 months) was used. Effects of the program were identified by comparing the results obtained by a group of inmates who had participated in the program (n = 80; experimental group) with those of another group who had received no intervention (n = 70; control group).
Results
The preliminary results suggested a certain treatment effect related to impulsivity and psychological distress.
Conclusion
Although the preliminary results were promising, the experimental and control groups did not differ significantly when more robust analyses were used.
Introduction
Four important facts have been established based on the current body of scientific knowledge on psychoactive substance addiction. First, a large proportion of inmates have addiction problems. 1 , 2 According to the profile of Quebec's correctional clientele drawn in 2007–2008, this is the case for 59% of Quebec inmates. 3 Second, the relationship between substance use and addiction, crime, recidivism, and re-incarceration has been clearly established. 4 Third, it is now recognized that correctional interventions developed and implemented according to established criteria reduce recidivism rates. 5 Finally, also established is the importance of prioritizing the development of integrated care systems that are flexible and that have the resources required to meet inmates’ needs both at the beginning and at the end of their substance use trajectory. 6
In Quebec, provincial institutions (prisons) administer sentences of 2 years less a day, while federal institutions (penitentiaries) administer sentences of 2 years and more. The services and programs offered differ considerably from one government level to the next, with federal institutions being better equipped. This article pertains to the provincial framework.
Incidentally, its continuation over the coming years is being funded by the Canadian Institutes of Health Research (CIHR), which will make it possible to obtain a more substantial base sample and perform more in-depth statistical analyses.
The purpose of selecting t-tests for the variance analysis was to minimize the attrition effect between measurement times on the results.
Studies pertaining to the effectiveness of correctional programs have led to the following broad principles that should guide correctional interventions intended to reduce recidivism: adhere to a psychological theory of criminal behavior5,7; abide by the principles of risk-need-responsivity 5 ; maintain integrity in program application and delivery8–10; and use the principles of the cognitive-behavioral approach7,11–13 as well as a team of engaged, qualified professionals.7,14 Prison-based addiction interventions aim also at reducing recidivism by decreasing substance use. 15 The following interventions are among those known to be the most effective: therapeutic communities,16–20 methadone maintenance treatments,6,19,21 as well as those applying cognitive-behavioral principles12,22 and motivational interviewing principles.23–25 Formal integration of aftercare has also proven advisable.18,26
Although research has shown that addiction treatment programs offered to inmates have real impacts on recidivism,27–29 to date, in Quebec, no treatment program specifically targeting these problems has been offered in provincial detention facilities 1 . 6 Consequently, having offered, since 2009, an innovative addiction intervention program as part of a socio-occupational reintegration school program, the detention facility in Québec City serves as a forerunner in the portrait of Quebec prison services.
This original intervention program was implemented at the Québec City detention facility thanks to an intersectorial agreement between the Ministère de l'Éducation, des Loisirs et des Sports (MELS, Ministry of Education, Recreation and Sports), the Ministère de la Santé et des Services sociaux (MSSS, Ministry of Health and Social Services), and the Ministère de la Sécurité publique (MSP, Ministry of Public Security), which helped combine their respective mandates and unite their efforts. Through the services offered in connection with the MELS social and occupational integration program, MSSS's Centre de réadaptation en dépendance de Québec (CRDQ) 30 provides the prison population with psychoeducational addiction services that adhere to the evidence-based principles of success. 9 Throughout the 6 weeks of intervention, inmates live in a department where they are isolated from the rest of the general prison population and which can accommodate a maximum of 14 people. The program relies on an integrated intervention approach31,32 and employs, on one hand, the harm reduction approach and,33–35 on the other, the cognitive-behavioral and motivational approaches.36,37 Therefore, through a mixed formula (alternating between therapeutic and academic activities), inmates are given the opportunity to pursue their studies while completing the addiction intervention program.
That said, although program evaluation plays a crucial role in the development of effective delinquent rehabilitation and reintegration programs,8,38 this practice is still neglected in Quebec's correctional system. 39 In the province's current sociopolitical context, carrying out a rigorous, empirical process of evaluating intervention programs poses major challenges, especially when the program falls under the responsibility of several government bodies,40,41 which is the case for the program under study.
There are numerous and varied determinants of substance abuse and addiction. Knowing that substance abuse and addiction problems are the result of the interaction between cognitive, psychological, and sociocultural factors particular to each individual, 31 as well as to the pharmacological properties of the substances consumed, 42 taking into account a comprehensive view of the individual is an essential a priori. The objective of the present study, which subscribes to this multidimensional view of the phenomenon, is to 1) assess the effectiveness of the CRDQ program offered at the Québec City facility. It will do so by 1.1) drawing a portrait of the substance use and of the psychological/emotional, social, and judicial spheres of the clientele admitted to the program, and 1.2) by measuring, at three time points (admission to the program, end of the program, and 6 months later), the changes that have occurred with respect to these same variables. Also documented are the services employed by participants in connection with their substance use problems, to gauge how well (or how poorly) they are managing in a change process and how much the program is appreciated by those who have completed it. Based on the criteria developed by the Substance Abuse and Mental Health Services Administration, 43 the following factors were selected to determine the program's success: significant improvement in the offender's psychological and social condition, significant improvement in the offender's Assessment and Screening of Assistance Needs (ASAN) 44 score between T0 and T2, and continuation of the aftercare process.
Method
This research project concerns quantitative data collected through repeated measures at three different time points (T0, T1, and T2) from volunteer participants comprising one experimental group (EG) and one control group (CG) 2 . Participants gave their written, informed consent to take part in the study.
Participant recruitment
EG participants (n = 80) were recruited among inmates who had joined the CRDQ program offered at the Québec City facility. To be admitted to the program, inmates had to meet the following selection criteria: 1) be a minimum security inmate; 2) have at least 6 weeks of detention left to serve; 3) have an alcohol/drug use problem requiring second-line intervention (moderate to severe level) in a specialized service according to the ASAN, a questionnaire designed to screen for and evaluate needs for assistance 44 ; 4) be motivated to start a process of receiving help; 5) be literate; and 6) be able to function in a group. People with a mental health disorder not controlled by medication were excluded from the program and, consequently, from the research project. Between November 2011 and October 2012, 96% of those newly admitted agreed to participate in the project.
CG participants (n = 70) were recruited at the detention facility in Trois-Rivières, where no program of this kind was offered. Having a sample from a prison population in another region helped us overcome the ethical obstacle encountered with impact evaluations: withholding an intervention from a part of the population whose condition requires it. 45 Having the CG and EG in different institutions also prevented contamination that could have occurred with two groups from a same facility, since Quebec prisons are too small for an EG and a CG recruited in a same location to be fully segregated. To participate in the research project, inmates in the CG had to meet all the criteria that would have been required for them to join the program at the Québec City facility, had such a service existed in their region. Further to a posting in selected sectors at the Trois-Rivières facility, inmates interested in participating had to advise a probation officer. The prison counselor then evaluated the files of interested inmates and selected those who met the selection criteria for EG participants in every respect. Although the ASAN requires a moderate or severe level of addiction for admission to the program, five inmates from the Trois-Rivières facility with lower severity levels were accepted into the CG because the crime for which they were incarcerated was directly linked to substance use – which was an exception clause for admission to the program.
Procedure
The T0 interview lasted an average of 90 minutes. EG participants were interviewed at the time of their admission to the program, and the CG participants when they expressed their interest. The T1 interview, which lasted an average of 45 minutes, took place 6 weeks after T0 (M = 44 days; SD = 8.14). These first two interviews were conducted face to face, at the detention facilities. The T2 interview, which also lasted 45 minutes, took place 6 months after the T1 interview (M = 201 days; SD = 30). It was held at the detention facility if the participant was still there; otherwise, it could be conducted face to face in a private and secure location (CRDQ, halfway house, Université du Québec à Trois-Rivières offices). However, in most cases, it was conducted by phone. Participants who were no longer inmates at T2 received financial compensation of $40. Figure 1 presents the number of participants at each time point as well as the time spread between interviews.

Participant follow-up by group.
Instruments
Substance use
We used a French version of the Addiction Severity Index (ASI), 46 the Indice de gravité d'une toxicomanie (IGT), which provides a biopsychosocial portrait of the person's situation based on seven spheres, four of which were used in this project, by calculating a “composite score” for each of them. This score enables us to quantify the participants’ degree of difficulty in each sphere. The IGT has been the subject of validation studies, which indicated good psychometric properties in terms of both validity (appearance and conceptual) and fidelity (test retest reliability, internal consistency). The key questions related to the alcohol and drug use sphere were used to meet objective 1.1. Assessment and Screening of Assistance Needs (ASAN)-alcohol/drug questionnaire 44 comprises an evaluation grid for estimating addiction severity based on three profiles (mild: first-line intervention needed; and moderate or severe: specialized intervention needed). The instrument includes the “Short Alcohol Dependence Data” (SADD) questionnaire, which is used for alcohol, and the Severity of Dependence Scale (SDS), which is used for drugs. The results from these scales were used to meet objective 1.2. The English versions of both scales have good psychometric properties47–52 and the internal coherence of QBDA and PDS have respectively, Cronbach alpha coefficients of 0.74 and 0.75 with an individual sample in specialized treatment of alcoholism. 53 Although not empirically validated, the DÉBA -A/D has been in use in the Quebec health network for nearly 12 years and has clearly crossed the stage in front of validity.
Psychological/emotional spheres
The key questions in the IGT Psychological Health Scale were used to meet objective 1.1, while the composite score (α = 0.71) from the same scale was used to meet objective 1.2. The following instruments were also used to meet objective 1.2 with respect to the psychological/emotional sphere: the Indice de détresse psychologique de Santé Québec (IDPSQ-14), 54 a questionnaire that measures psychological distress levels according to four types of symptoms (depression, anxiety, irritability, and cognitive problems); the Barratt Impulsiveness Scale (BIS11), 55 which evaluates impulsivity-related personalities and behaviors; and the Questionnaire sur le pouvoir d'agir personnel (MAPS20), 56 which includes four subscales (self-esteem, life goals, internal locus of control, and sense of self-efficacy). Préville (1994) evaluated the reliability and validity of the IDPSQ-14 and found that it had a significant concurrent validity (internal consistency of 0.89). Meanwhile, the BIS11 has a long tradition of research and a proven factorial validation. 57 Internal consistency analysis revealed a standardized Cronbach's α = 0.81. Finally, during a validation study of MAPS20, α's obtained are from 0.58 to 0.86.
Social sphere
The key questions from the IGT Family/Interpersonal Relations scale were used to meet objective 1.1, while the composite score (α = 0.63) from the same scale was used for objective 1.2. Also used for objective 1.2 was the family and friend version of the Perceived Social Support Questionnaire (PSS Fm/Fr), 58 which assesses how the individual's needs for support, information, and feedback are filled by friends and family. This instrument has been translated into French and validated with a Quebec population. 59 Internal consistency analysis revealed a standardized Cronbach's α of 0.78 for the family and a 0.74 scale for friends.
Judicial sphere
The liaison officers from each detention facility filled out a sociodemographic data sheet (CRDQ) based on information from the correctional file. The resulting data were used to draw the participants’ portraits, to meet objective 1.1. The composite score (α = 0.75) from the Judicial Situation scale in the French version of the Addiction Severity Index was used for objective 1.2.
Services used
With respect to objective 1.2, the following instruments were used to document the services used and the continuation, or lack thereof, of a care process: the in-house questionnaire on Services Used (1 year before T0, between T0 and T1, between T1 and T2); the questionnaire on Perceived Improvements (CRDQ), to assess the level of satisfaction regarding the various aspects of the program and the perceived changes by life sphere since completion of the program; and the Questionnaire sur la motivation au changement (QMC), 60 which summarizes the dimensions of the motivation-to-change model 61 and helps determine which stage the subject is at. In a validation study conducted with an adult population, the authors of the original version of QMC obtained acceptable α's 62 between 0.73 and 0.85.
All questionnaires except for the IGT, the DÉBA-Alcool/Drogue, and the one on perceived improvements were administered at every time point, for the EG and the CG alike. The complete version of the IGT was administered only at T0, while the abridged version was used at T1 and T2. The ASAN-Alcohol/Drug was administered only at T0 and T2, to both groups. Finally, the questionnaire on perceived improvements was administered only to the EG, since it concerned the participants’ appreciation of the services received.
Statistical analyses
The statistical analyses were performed in three steps. First, descriptive statistics was conducted, based on the data collected at T0, to draw a portrait of the participants divided into the two groups, in regard to substance use, the psychological/emotional sphere, the social sphere, and, finally, the judicial sphere (objective 1.1). Independent sample t-tests and chi-square tests were conducted on target variables to verify the levels of homogeneity of the variances for the two groups. Second, matched t-tests (T0–T1; T1–T2; T0–T2) for each group (EG and CG) and independent sample t-tests (T0, T1, T2) were carried out to measure within- and between-group changes 3 , with regard to substance use, the psychological/emotional, social, and judicial spheres, as well as the care process (objective 1.2). Finally, based on the most promising t-test results, latent growth curve analyses 63 were conducted to find out whether an effect directly related to group membership would emerge from the results.
Results
Participants’ Portrait
Table 1 presents the participants’ main sociodemographic characteristics by group. To ensure equivalence of the groups, the criteria for inclusion in the program were rigorously applied for the selection of CG participants. Because the program evaluated is offered only to the male prison population, the sample is composed only of men. Table 1 shows that participants were with a mean age of 36 years and received, on average in their life time, 4.77 sentences (EG: 4.05; CG: 5.49). So, they still averaged 27.25 months purged (EG: 25.03; CG: 29.48) during their lifetime. Quebec provincial prisons authority is responsable of those sentenced to incarceration time of lest than two years, the average duration of the currently incarceration is 380.65 days (EG: 374.43; CG: 386.86).
Participants’ sociodemographic characteristics by group.

P < 0.05;
P < 0.01;
P < 0.001.
Although most of the participants’ characteristics presented in Table 1 are similar for both groups, CG participants present a slightly more vulnerable portrait than EG participants, in terms of the following variables: they had consumed cocaine and cannabis regularly for a significantly longer time; they had received significantly more treatments for drug use in their lifetime; they had been given more sentences, on average, in their lifetime; and, finally, a larger number of them had been physically abused.
Evolution of the participants’ psychosocial situation across time points
Among the criteria for inclusion in the program, inmates must have had at least still 6 weeks to be served within the walls so that they were able to follow the whole program. However, it happens that some inmates were excluded from the program for various reasons (behavioral problems, violence against other inmates, being involved in drug trafficking inside the walls, etc.). As part of this study, only three inmates were excluded from the program after 4 (n = 2) or 5 (n = 1) weeks. As part of the program had already been completed by them, they were still invited to the three time points.
Table 2 presents the participants’ scores, by group, for the various questionnaires.
Participants’ scores, by group, for each questionnaire.

Table 3 presents the results of the comparative analyses of the means, that is to say, for each group between the various time points, to check for any improvement or a deterioration in the participants’ situation across time; and between the groups at each time point, to check for differences between the EG and the CG for any of the spheres.
Evolution of the participants’ situation by group, across time points, and comparison between the groups by time point.

P < 0.05;
P < 0.01;
P < 0.001,
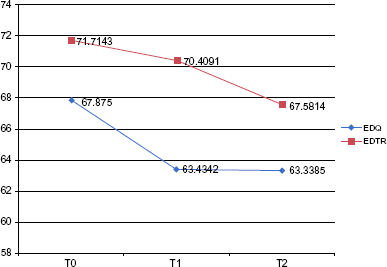
Initially, the IDPSQ and BIS11 results appeared to be the ones related to the treatment effects. As illustrated in Figure 2, the IDPSQ results showed that, when the two groups were compared, EG participants presented lower levels of distress than CG participants at T0. Between T0 and T1, the EG had a significant decrease in psychological distress, which maintained the significant difference between the two groups at T1. However, with psychological distress of the EG increasing between T1 and T2 and that of the CG decreasing significantly between T0 and T2, the two groups no longer differed at T2 with respect to this indicator.

IDPSQ results.
The BIS11 results, as illustrated in Figure 3, showed no significant difference in impulsivity levels between the two groups at T0. However, because of a significant decrease in impulsivity between T0 and T1 for EG participants, the two groups were significantly different at T1. A comparison between the scores obtained at T0 and T2 showed an improvement (decrease in impulsivity) for both the CG and the EG. Nonetheless, at T2, EG participants remained significantly less impulsive than CG participants.
BIS11 results.
The latent growth curve model 63 was used to estimate the variation in psychological distress and impulsivity between the first and second time points, based on the following hypotheses: Y[t] = y0,n + ys,n x group[t]n + e[t]n; y0,n = μ0 + d0,n; and ys,n = μs + d s,n. In the first model, the tests were performed without consideration of membership in the EG. These models did not fit the data: distress: X 2 = 11.520, df = 1; P < 0.001, and RMSEA 90% CI = 0.143–0.411; impulsivity: difference X 2 = 1.744, df = 1; P > 0.05, and RMSEA 90% CI = 0.000–0.242. Additional tests were then conducted on the models by fixing the slope variance at 0, suggesting an identical variation for all participants. The results for psychological distress are presented in Figure 4, and for impulsivity in Figure 5. In both cases, no conclusion could be drawn regarding a treatment effect.

Path diagram of IDPSQ results.

Path diagram of BIS11 results.
Questionnaire on perceived improvements
As mentioned above, the questionnaire on perceived improvements (CRDQ), with respect to services received, was administered only to EG participants at T2. The results indicated a relatively high level of satisfaction. For the various program-related aspects, 84% of participants said they were “very” or “extremely” satisfied. It should be noted that “listening, respect and assistance from the personnel,” “quality of services received”, and “services received overall” stand out, with satisfaction rates of 95%, 91%, and 91%, respectively. The results were promising with regard to the participants’ evaluations of various spheres of their lives after their move to the specialized department, since 92% of participants believed that their overall situation was “better” or “much better” than before the program. The alcohol and drug use spheres had improved for 71% and 63%, respectively, of the participants. Psychological/emotional health and relationships with people in their circle had also been positively affected for 77% and 58%, respectively, of the participants. Regarding the judicial sphere, 92% of participants felt their involvement in criminal activities had decreased, and 75% deemed their judicial situation improved. Meanwhile, 27% of participants said they had seen no change in the various spheres since completing the program. However, it should be noted that, among them, 76% said that the sphere in question had not been problematic even before they had joined the program.
Discussion
As part of this research project, the team set up as exhaustive an evaluation as possible,64–67 considering the realities specific to the prison context and the marginalized population it serves. 40 The program under evaluation adhered to the fundamental principles of effective addiction intervention 68 in prison settings.5,7,13,69 In the end, the results of the preliminary analyses suggested a certain impact of the program on participants’ psychosocial situation, notably with respect to impulsivity and psychological distress. That said, despite all these considerations, the demonstration based on more robust statistical models did not lead to any conclusion regarding the effectiveness, or even the ineffectiveness, of the CRDQ program offered at the Québec City facility. Findings were the same for other researchers,70–73 who had also conducted program evaluations in prison settings. These results, which can be explained by various elements – of a conceptual or contextual nature, or related to the prison clientele – still help to draw broad conclusions regarding addiction intervention and program evaluation in a particular context.
First, the conclusions from this research project support the already vast body of evidence showing that addiction is a multidimensional phenomenon that, like other social issues, resists the medical experimental model, which is still considered the main foundation for the so-called evidence-based results.74,75 We believe that the results presented here are an indication of the limitations of a purely linear evaluation, with pre and postintervention measures, in terms of drawing conclusions as to the effectiveness of an addiction intervention. That said, although addiction is a transitory problem that will be resolved by a spontaneous or natural remission for some users, 76 the fact remains that it is a chronic problem for others. 77 In the guide published by the National Institute on Drug Abuse (NIDA), 78 where it lists the 13 principles of addiction treatment for the criminal justice population, the Institute recognizes that numerous episodes of treatment are generally needed for this multi-problem clientele. It thus seems that an accumulation of episodes of care is generally the norm rather than the exception, and that an average of three to four episodes, spread over several years, is usually required to achieve sustained abstinence. 79 This accumulation of services makes it difficult, if not impossible, to differentiate between the benefits gained in each of the services used and, even more so, to attribute the success indicators to one service or another.
It is recognized that practical, administrative, legal, and ethical challenges related to the prison context make it impossible to adhere to fundamental research standards, such as single blinding, double blinding or randomized testing.80,81 That is why, in most cases, criminology researchers turn to a quasi-experimental design, 82 which remains the best alternative for maximum validity 83 when an experimental design is impossible, difficult, or simply inappropriate.84–86 The major challenge remaining with this type of design is related to group equivalence. 75 The more similar the groups, especially in terms of personal characteristics related to the program intervention, the more the results are considered reliable. 87 In this project, despite a rigorous selection of the CG participants in accordance with the same program inclusion criteria as those imposed on the EG participants, the results of the statistical analyses showed, at the outset, certain between-group differences that are likely to have influenced the results. Furthermore, in this type of research design, certain key variables are difficult to control, statistically or through matching, and lead to bias in the results, despite all the precautions taken by the researchers. 88 For example, contrary to a scientific laboratory where everything is controlled, subjects in the CG remain in prison, which is not sanitized of all social contacts (correctional officers, probation officers, chaplain, professors, etc.), likely to influence their substance use trajectory8,69 even if they are not in any program. In this regard, recent studies on treatment effectiveness demonstrate how important the quality of the therapeutic alliance is in explaining why a therapeutic process is successful or not. 89 We did not measure this variable in our study, and it goes without saying that alliances would have developed in prison, in both the EG and the CG, and that they might have influenced the evolution of the person's situation. Moreover, the fact that the post-incarceration period can be part of the design for some participants is another element that is difficult to control for researchers and that can influence the results. Lösel points out that these methodological difficulties are the result not of the researcher's lack of knowledge but rather of the constraints of the environment that interfere with or prevent the use of the optimal design in regard to the research objectives. 90
The fact that the program is dispensed in a provincial detention facility also poses its share of challenges, in terms of service availability and evaluation, notably because of the duration of the sentences served in these facilities. Among the persons incarcerated in a provincial facility in 2010–2011, 64% were serving a prison sentence of 6 months or less. 91 Stewart believes that short sentences considerably complicate the processing of inmates’ files (evaluation, referral to services) and often result in inmates being inadmissible to intensive services. 92 They are thus, according to Kivivuori and Linderborg, unfortunate victims of an “under-supply” of services. 93 These short sentences would also have an impact on inmates’ motivation to begin a program in detention, not seeing the point of doing so, often because of their imminent release. 94 In this context, the offer of an intensive 6-week program is noteworthy and is testimony to the partners’ sincere desire to meet their clientele's needs. In this regard, although not all studies agree on the optimal duration of an internal program, the trends show that a 28-day treatment would be more effective than a 10-day or 60-day one. 95 Nonetheless, it is important to mention that during the 6 weeks of treatment, inmates divide their time between academic activities (50%) and therapeutic ones (50%), and that addiction caseworkers are absent in the evenings and on weekends. Therefore, the actual treatment duration is at the limit of best practice recommendations, which may not be enough for real changes to occur for such a complex problem, and undoubtedly limits the possibility of detecting clearly significant results.
Just like in addiction services, the “revolving door” phenomenon is present in the provincial prison system. Again, in a provincial institution in 2010–2011, it was estimated that inmates had been given, in their lifetimes, an average of six detention sentences of less than 6 months. 91 Considering this clientele's average age of 37–38 years, we can conclude that a number of provincial inmates go back and forth frequently and in rapid succession between prison and the community. Partnership with the community thus becomes paramount. 91 Again, according to NIDA principles, 78 people who complete a program in detention and receive continuing care in the community achieve better results. Treatment in the community thus becomes essential for maintaining the progress made in prison. It is important to acknowledge and emphasize the innovative and rather daring nature of the partnership between three government departments as part of this program. However, it is imperative that the continuity of this initiative within the community be at the heart of the partners’ concerns, to maximize longer term outcomes, since the evidence shows that follow-up on the outside is just as important as the duration of the treatment on the inside. 96
Furthermore, with the introduction of the harm reduction principle, to which the program under study adheres, treatment effectiveness has become far more intricate and realistic; it no longer boils down to achieving abstinence alone but rather to a decrease in the negative consequences of substance use, for the addicts and the people in their circle.33–35 Consequently, the results can sometimes be more difficult to demonstrate statistically. Moreover, the research context inherent to prison settings means that the success of an intervention is interpreted very differently depending on whether statistical or clinical criteria are used. 97 Therefore, as the effectiveness of a program varies according to the outcomes measured, 96 both aspects must be considered in the program evaluation, in the most inclusive perspective possible. In the case at hand, there are no statistically significant variations; however, the fact remains that 65% of inmates in the EG felt that several spheres of their lives had improved following the program. The addition of a qualitative component focusing on user satisfaction would have been shown in such gait and would probably brought an interesting light on the assessment of more subjective parameters such as the real effects, felt and perceived by the program users.
The incarceration period is an opportune time for addicted inmates to be offered services related to their substance-use problem. 6 Even though attitude changes do not always translate into behavior changes 69 – as is expected of long-term designs, which are often very, or even too, onerous in the current context – awareness and increased motivation are part of one of the steps in a rehabilitation process that will ultimately lead to long-term maintenance of the progress made and are encouraging outcomes in themselves.
Author Contributions
Conceived and designed the experiments: CA, MA, CP, FF, NBM. Analyzed the data: CA, MA, MR. Wrote the first draft of the manuscript: CA, MA, C P. Contributed to the writing of the manuscript: CA, MA, CP, FF, NBM. Agree with manuscript results and conclusions: CA, MA, CP, FF, NBM, MR. Jointly developed the structure and arguments for the paper: CA, MA, CP, FF, NBM. Made critical revisions and approved final version: CP, FF, NBM.
Ethics
This project was approved and authorized by the Addiction Research Ethics Committee of the Ministère de la Santé et des Services sociaux, the Human Research Ethics Committee of the Université du Québec, and the Research Branch of the Ministère de la Sécurité publique. The research was conducted in accordance with the Declaration of Helsinki.
Footnotes
Acknowledgments
They also thank the liaison officers Nancy Corriveau (EDTR) and Katrine Ouellet (EDQ), without whom the success of this project would have been greatly compromised. Finally, special thanks to all the participants, who generously agreed to share their experiences and without whom this project would have never existed.