
Abstract
Uncovering patterns of drug use and treatment access is essential to improving treatment for opioid dependence. The life history calendar (LHC) could be a valuable instrument for capturing time-sensitive data on lifetime patterns of drug use and addiction treatment. This study describes the methodology applied when collecting data using the LHC in a sample of individuals with long-term opioid dependence and aims to identify specific factors that impact the feasibility of administering the LHC interview. In this study, the LHC allowed important events such as births, intimate relationships, housing, or incarcerations to become reference points for recalling details surrounding drug use and treatment access. The paper concludes that the administration of the LHC was a resource-intensive process and required special attention to interviewer training and experience with the study population. These factors should be considered and integrated into study plans by researchers using the LHC in addiction research.
Introduction
Opioid dependence is a chronic illness, characterized by patterns of continued drug use and intervening periods of treatment, abstinence, and relapse. This condition remains a significant public health challenge and poses great harms to the individual, her/his family, and the community, particularly when untreated.1,2 Patterns of drug use,3–5 victimization,6,7 health outcomes,5,8 and treatment access 7 in this population have tremendous implications for the provision of care for men and women struggling with drugs.
While previous studies with opioid-dependent men and women have investigated patterns of drug use and treatment access, many of these studies have relied on questionnaires or standardized instruments that tend to overlook lifetime experiences related to opioid dependence. 4 ,8–11 Obtaining a complete picture of a person's patterns of drug use and treatment access might not be attainable with such tools. Calendars and timelines are alternative methods to collect lifetime data in order to explain relationships between complex lifetime events. 12
Calendar and timeline methods have shown to have a range of advantages when compared to traditional questionnaires. 13 The life history calendar (LHC) increases the completeness of reporting of events as its graphical display of time allows respondents to better access long-term memory, and allows interviewers to identify “gaps” in reported data. 14 The displaying of distinct events as part of a larger sequence facilitates memory recall.14,17 Respondents are able to relate events from different life domains to each other, improving the timing of specific events. This is particularly useful for recalling less recent, more frequent, and less salient events. Further, empirical evidence has shown that the LHC method works to enhance the consistency of responses and reduce recall error common in retrospective data, such as dating error and omission.13,15
The LHC collects information on lifetime events identifying patterns, co-occurrences of significant life events, and landmarks over a life course and has been shown to be an effective form of gathering information and capturing important transitional periods.13,16 The LHC improves the quality of the reported retrospective data, by helping the participant relate, both visually and mentally, to the timing of several kinds of events. 17 Life event calendars are used in health or social surveys to obtain lifetime patterns that complement cross-sectional associations.18–20 Some retrospective studies have included questions in the life calendar regarding substance use as one of the factors that could explain the health or social outcome of interest. 20 In addiction research, specifically, the calendar has been mostly used to collect daily patterns of substance use, with a follow-back time period, usually of one month.21–23
Although the LHC has been used to measure patterns of substance use among various groups,18,20,24–26 to our knowledge, the feasibility of administration within a population of long-term chronic opioid users has not been investigated. Drug use and treatment variables assessed in combination with one another and over a lifetime reference period with the LHC could reveal patterns and underlying mechanisms that have strong implications for the provision of care for men and women struggling with opioid dependence.
This paper aims to describe the methodology applied when collecting data using the LHC in a sample of individuals with long-term opioid dependence and to identify specific factors that impact the feasibility of administering the interview. Further, the paper aims to discuss the potential role of the LHC in addiction research.
Methods
Design, setting and participants
The LHC was collected as part of a descriptive mixed-method cross-sectional pilot study. The GeMa (gender matters in the health of long-term opioid injectors) study aimed to identify gender-specific patterns in drug use, victimization, access to care, and physical and mental health among men and women with long-term opioid dependence. The study was conducted in Vancouver, Canada, between December 2011 and July 2013 by a research team with a longstanding and consistent presence in the community. Recruitment strategies included referral through community-based health-care organizations, other research studies with a similar target population, and word of mouth. Inclusion criteria for GeMa consisted of the following: (a) 19 years of age or older (adult age in British Columbia); (b) residing in the greater Vancouver metropolitan area; (c) at least 5 years of opioid use prior to participation; (d) regular use of illicit opioids during the six months prior to participation; and (e) one or more episode[s] of methadone maintenance treatment (MMT) or another form of opioid substitution treatment (eg, Suboxone). A total of 178 individuals participated in the study (male = 95; female = 80; transgender = 3); 56 of whom completed the LHC (male = 33; female = 22; transgender = 1). All research procedures were reviewed and approved by the Providence Health Care/University of British Columbia Research Ethics Board. This research complied with the principles of the Declaration of Helsinki.
Eligible participants met at the confidential research office, and the informed consent form was reviewed and signed prior to any data collection. During this visit, questionnaire data were collected on the following topics: (1) socio-demographics; (2) intimate relationships; (3) pregnancy and parenting; (4) sex work; (5) substance use; (6) physical health; (7) mental health; (8) health-related quality of life; and (9) history of victimization. At the end of this visit, participants were invited to complete the LHC on a separate visit.
Life history calendar
After completing the questionnaire package, participants were invited to do the LHC. Those who accepted scheduled an appointment to return on another day (usually the next day, never more than one week from the date the questionnaire was completed). Interviews took between 30 and 60 minutes, and participants were provided a stipend for their time. Two trained and experienced inter viewers, both with bachelor's degrees in a health-related discipline and prior experience working with underserved populations, administered the LHC. A multiphase training process was used to ensure that the interviewers had strategies to engage the participant in the interview, understood the variable definitions, the technical aspects of the spreadsheet, and navigation of the coding sheet. Both interviewers also conducted a mock interview prior to administering the instrument.
The LHC covered the same topics as the GeMa questionnaires (Table 1). However, the LHC collected data in a unique format meant to reveal time-linked relationships between the variables of interest.15,17 A lifetime reference period was chosen to capture early experiences that might have preceded, co-occurred, or resulted from illicit opioid use and addiction treatment (ie, victimization, housing), the primary variables of interest. Patterns between variables could be mutually exclusive (eg, in jail/not in jail) or concurrent (eg, on methadone and also using illicit opioids).
Topics, variables, and example codes used in the LHC.

Data were recorded electronically on a grid style spreadsheet (Fig. 1). The participant and interviewer sat beside each other with the study laptop open displaying the calendar. At the start of each interview, the participant's date of birth was entered into the spreadsheet, which automatically formatted the spreadsheet so it populated each month and year from participant's birth to the interview date. The birth month of each year was also automatically highlighted for reference during the interview. For each variable, codes were developed to describe participants’ responses (Table 1). These codes were entered into the corresponding cells of the variable for the referent month.

Example of grid style spreadsheet.
Administration of the Lhc in the Gema Study
Format of the LHC
The computerized spreadsheet and the side-by-side position between the interviewer and participant provided a visual representation of the timing, gaps, sequence, and relationships between variables. In addition, the structure of the LHC spreadsheet allowed the interviewers to quickly tailor the calendar to include variables of relevance to the participant by expanding and collapsing the variables. This visual format engaged the participant in the collection process and has also been shown to be effective for aiding memory recall.14,17
Reference period
In this study, a lifetime reference period reliably identified ‘firsts’ (ie, marriages, birthdates of children). However, participants’ ability to recall the month and year of specific life events or behaviors was almost impossible. If this information was collected, responses were usually vague (eg, “I don't know. October.” or “I don't know, sometime in the summer.”). If the participant could not remember the exact month and/or year of an event, the interviewer recorded the event in the closest month or year it could be recalled. If participants could only remember the age at which an event occurred and not the month, date of birth was used for data entry.
Previous research using the LHC has shown high correlations on test–retest reliability for general information and key events (eg, employment, child births, school attendance),16,27 but agreement decreased when participants were asked more information surrounding specific tasks or behaviors. Reliability decreased even further when asked about specific times (ie, days, weeks).16,21,27
The lifetime reference period in calendar-style instruments is an important methodological decision, and benefits and drawbacks should be considered during the design phase. A critical benefit of our LHC design was that the data would identify developmental events, behavior patterns, milestones, and transitions that may influence their patterns of illicit opioid use and access to addiction treatment. A drawback is the reliance on retrospective recall, increase in the duration of the interview, and the subsequent effect of these on the physical and emotional state of the participant.
Assisting memory recall
Two interviewer techniques assisted in memory recall and facilitated accuracy of responses: (1) the use of anchor points and (2) reference to life events reported in the questionnaires. Anchoring is a technique frequently used when collecting information retrospectively to facilitate recall of specific activities, behaviors, and events. 13 In our administration of the LHC, interviewers asked the participant questions about general events or time periods (ie, birth of a child, employment histories, housing, and marriages) to aid in the memory recall of specific events (ie, age of first heroin use, incarcerations, diagnosis of a chronic illness, and attempts on MMT). For example, if a participant had trouble recalling their housing situation during a certain time period, but could recall with certainty a period of incarceration or length of time they used heroin, interviewers used these known events as anchors.
Significant life events were ‘participant defined’ rather than ‘researcher defined’ increasing the overall effectiveness of the technique and reliability of the information collected. For example, one participant could not remember the first time he received addiction treatment, but was able to recall in detail the year, month, and charge of his first incarceration. Another could not remember the year she got married, but could remember the year she injected heroin for the first time.
The complementary data collected in the questionnaire package provided the interviewers with background knowledge of the participants’ histories that was used to support or ‘fill in’ data during the LHC administration. Reference to the participants’ histories improved the flow of the interview, aided in memory recall during the LHC, and eased the memory work required by the participant.
The following interview scenario illustrates the use of the anchoring technique and the resulting participant response pattern:
Interviewers kept the primary research question in mind during the interview and consistently related life events back to the dependent variables. For example, if the participant reported a period of incarceration, the interviewer would follow-up, “and when you were in jail, what happened to your drug use. Did you stay on methadone or did you keep using heroin while in jail?”
Interviewer role
While administering the LHC, four major aspects of the interviewers’ use of the LHC positively impacted the quality of the data collected. First, the training of the interviewers and the scoring card maintained the consistency of the interviewers’ data collection. Second, attention to detail was important to ensure that data were recorded in the correct variable line of the spreadsheet (with a lifetime of 40 years it can be difficult to follow). Third, the interviewers reviewed the data collected in the calendar immediately after completing the interview (after the participant left). This strategy improved accuracy and reduced data loss. Fourth, interviewers were familiar with events that commonly co-occur in the study population, which permitted asking appropriate questions to fill in or identify gaps in the LHC. For example, if the participant reported regular cocaine use from age 15 to 21, but was in jail for 6 months at the age of 18, the interviewer had the contextual knowledge to question what happened to the cocaine use during the period of incarceration. This knowledge and attention to detail reduced potential errors from over-reporting and data entry.
In addition to proficiency in the use of the LHC technically, several interviewer characteristics were critical to collecting LHC data with an opioid-dependent population. During interviews, participants often experienced cognitive and physical symptoms associated with substance use (eg, fatigue, opioid withdrawal, physical injuries). Interviewers were attentive to the emotional and physical state of the participant in efforts to provide a respectful atmosphere and maintain quality of the data. In these situations, interviewers balanced the pressure to administer the LHC more quickly to accommodate the needs of the participant, while being careful not to risk the quality of the data. Sometimes the interview was rescheduled.
Interviewers were also careful not to introduce their potential assumptions about a participant's history as this might be offensive, discourage disclosure, and negatively affect the dynamic of the interview. This was especially relevant as our LHC included sensitive topics, such as involvement in criminal activities, histories of victimization, and child apprehensions. The sensitive nature and perceived stigma of these topics might have led to under-(eg, illicit income and employment) or over-reporting (eg, relationship with child) of some events. To reduce this likelihood, the study's interviewers demonstrated empathy, non-judgmental response, patience, and respect toward participant boundaries.
Analyzing the LHC
Data from the LHC spreadsheets produce individual plots (Fig. 2), which display the participant's age chronologically and the occurrence of the life events. The main variable of interest, illicit opioid use, is displayed in the top half of each plot so the patterns, timing, and sequence of the relationship between the variables can be seen visually. This visual representation has been useful for examining the quality of the data collected, to identify gaps and inconsistencies.
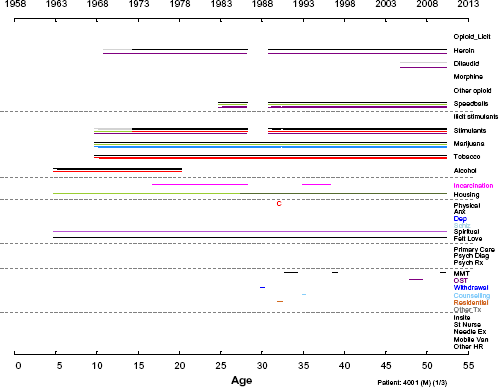
Example of individual plot.
The plots illustrate how the LHC data can answer research questions that would have been missed using only questionnaires. For example, a key question of interest to our team is what events are associated with stopping or reducing illicit opioid use during periods of treatment. The LHC collected data on the use, frequency, and intensity of illicit opioids for each month in the participant's life, capturing transitions. Data collected in this way will allow us to determine the specific treatment attempts where transitions in illicit opioid use occurred and what life events are associated with these transitions. While our study questionnaires asked participants to recall the number of months participants were abstinent of illicit opioids while receiving treatment, this question alone does not capture other important data, such as changes in the pattern of use, the treatment periods affected, the timing of the transition, or the order of the transition.
Limitations
The design of the present study did not include a psychometric assessment of the LHC. The LHC was administered in a one-on-one interview by two different interviewers but only once with each participant; thus, inter-rater reliability and test–retest reliability were not addressed in this study. Also, the data collected in the LHC were self-reported, and objective measures of validity (eg, urine drug screens, health records, criminal records) to possibly verify participants’ responses were not taken. Nevertheless, it has been suggested that objective measures and self-report data complement rather than validate findings. 28 Moreover, research has consistently shown that self-report data among drug users are consistent and reliable when research is conducted by staff with no agency on participants’ clinical care 29 such as the case of this study.
Conclusion
To our knowledge, this is the first use of the LHC with individuals with chronic opioid dependence and in reference to a lifetime period. Most of the participants had experienced several treatment attempts, and alternating periods of drug initiation, abstinence, and relapse. The LHC's lifetime reference period allowed important events such as births, intimate relationships, housing, employment, and incarcerations to become reference points for recalling details surrounding drug use and treatment access. Data from the LHC could explain relationships between these complex lifetime events otherwise not captured with questionnaires. Uncovering these complex relationships could inform timely interventions and prevent relapses.
Nevertheless, while first time events were well recalled, more detailed histories required more effort to be obtained. Also sensitive topics, often related to drug use transitions, require time and effort to work out. Since the application of the LHC with long-term opioid users could be resource intensive, researchers should consider a number of variables that fit the length of the interview or plan for several appointments (with the inherent risk of missing data for participants not returning to complete the interview).
The application of the LHC requires special attention to the interviewer training, role, and experience with the study population and topic. In this study, many sequences of events required the interviewer's knowledge to ask the proper questions to fill the gaps. The LHC complemented a questionnaire package with the aim of collecting rich data in a sub-sample. The interviewers’ cognizance of participants’ responses to the questionnaire package facilitated the completion of the LHC. Therefore, addiction researchers should consider budgeting for training and investing in a stable team throughout the project.
Author Contributions
Conceived and designed the study: EOJ. Analyzed the data: JF, KM, HP, EOJ. Wrote the first draft of the manuscript: JF, EOJ. Contributed to the writing of the manuscript: KM, HP. Agree with manuscript results and conclusions: JF, KM, HP, EOJ. Jointly developed the structure and arguments for the paper: JF, KM, HP, EOJ. Made critical revisions and approved final version: JF, KM, HP, EOJ. All authors reviewed and approved of the final manuscript.