
Abstract
Background
Women in opioid maintenance treatment (OMT) have a past characterized by drug abuse, which is a challenging start for parenthood. Studies of mothers in OMT are typically limited to pregnancy and early infancy. Knowledge about how they cope with substance use and related problems in the years following birth is therefore important. The aims of the study were to examine changes in mothers’ substance use, psychological problems, and other challenges; from one to four years after their children were born, and describe kindergarten attendance and prevalence and type of child protective services involvement when the children were four years old.
Method
A four-year prospective cohort study of mothers in OMT. The European severity index was used to map substance use and related problems during the third trimester of pregnancy, one and four years after birth.
Results
At the four-year follow-up, use of illegal substances remained low (4%) and use of legal substances (39%) was similar to the one-year follow-up. The proportion of women with psychological problems was significantly higher than at one-year follow-up (69 vs. 39%, P = .009). At age four, most children (89%) attended kindergarten, and the child protective services were following 73% of the families, mostly with voluntary measures.
Conclusion
Mothers in OMT cope well with substance use over time, given access to sufficient support. The findings imply that a preventive governmental strategy with close support of mother and child, have a positive impact contributing to making OMT and motherhood more compatible.
Introduction
While opioid maintenance treatment (OMT) has been used for about 50 years and WHO recommends this treatment for pregnant women who are opioid dependent, 1 some practitioners and politicians have raised concerns.2–7 Therefore, prescribing OMT to pregnant women and mothers remains controversial. The current body of research is focused on pregnancy and infancy; to address the concerns raised and to design policies that support these mothers as the children grow up, a longer perspective is needed and knowledge about how they cope with substance use and related problems in these years is important.
OMT patients have a background of heavy substance use, often accompanied by psychological problems, problems with family and friends, unemployment, and legal problems;8–11 opioid dependent women who become pregnant are no exception. OMT has been effective in reducing the use of illegal substances, also among opioid dependent pregnant women and mothers.12–14 However, little is known about mother's substance use and related problems beyond pregnancy and infancy.
The proportion of mothers in OMT with psychological problems is high, and having young children often leaves little time for them to deal with their own problems. 15 Further, serious conflicts with family and friends, or legal problems, take away much of the attention and focus that should otherwise be dedicated to their children. 16 While previous studies have described these issues in pregnant women in OMT and during infancy,12,15,17,18 knowledge beyond this period is limited. Investigating how psychological and other problems develop among these mothers as their children grow older is therefore important.
At the time participants were recruited to this study, the national OMT program in Norway was a high-threshold program with strict inclusion criteria, rigorous control, and frequent urinary drug screening.13,19 The inclusion criteria were: >25 years, 5 or more years of opioid dependence, the patient must have tried non-medication oriented treatment, and had to be accepted into the program by regional OMT centers. Up until 2011, approximately 300 children were born to mothers in OMT in Norway. 20
The Norwegian law on substance use during pregnancy is very strict, with a zero tolerance to substance abuse during pregnancy. Treatment providers are obliged by law to take action if women continue to abuse drugs and/or alcohol. In cases where voluntary measures to stop such abuse does not help, women may be detained in in-patient treatment facilities, with or without their consent, for parts of or the entire pregnancy. 21 The rationale behind this is to reduce the risk of negative birth outcomes, such as malformations, which continued substance use may contribute to. 21
While appropriate support benefits the mothers and their children;22,23 the extent and type of support vary from country to country. The welfare state in Norway ensures all inhabitants are covered by a free national health care system. Confounding factors such as extreme poverty and homelessness, which often accompany drug abuse, and contribute to poor treatment outcomes 24 hardly occur in the Norwegian setting, where housing is offered and paid by the state for individuals unable to cover these costs. This includes individuals with substance use or psychiatric problems. 20 National guidelines for pregnant women in OMT describe the extensive support they receive from pregnancy until the child starts school. 20 For example, governmental support includes support covering the costs of kindergarten attendance or respite care. The national guidelines also suggest that the child protective services should participate in the support of the families from an early stage, often starting during pregnancy, and in the absence of continued substance use or other severe issues, they cooperate with the families about early and proper assistance; aiming at children growing up with their parents. 20
Previous studies of mothers in OMT and their children have followed them in the infancy period, 25 or used strict inclusion criteria; excluding for example women who were using alcohol or benzodiazepines. 26 To investigate how they are doing over time, as their children grow older, prospective studies are necessary. The Norwegian cohort of mothers in OMT and their children is the first of its kind; all pregnant women in OMT were invited to participate in the prospective study, which achieved a high participation rate. Previous studies on the cohort have described fetal and neonatal outcomes in children exposed to methadone or buprenorphine in utero, 13 ,27–31 substance use and psychological problems among mothers during pregnancy and one year after the children were born.12,15 There was little use of both illegal and legal substances during pregnancy, but a tendency to increased use of legal substances (alcohol and benzodiazepines), and reduction in psychological problems one year after the children were born.12,15 It remains to be seen if this pattern changes over time. Knowledge arising from this prospective study will help fill the knowledge gap regarding substance use and related problems over time in this group. This knowledge is also relevant in both clinical and policy settings.
Given the high control and close support setting of Norwegian OMT, the purpose of the study was to (1) examine changes in mothers: substance use, psychological problems, and other challenges; from one to four years after their children were born, (2) describe kindergarten attendance, prevalence, and type of child protective services involvement at the time when the children were four years old.
Method
Participants
Between 2004 and 2006 all pregnant women in OMT in Norway were invited to participate in a prospective study. Of the 47 women, 41 agreed to participate. Of the six who did not participate, four said they did not want more health care personnel and researchers involved in their lives, and two women reported their partners were skeptical of the study and that they therefore did not want to participate. Of the 41 who agreed to join, two women dropped out because of miscarriage and one withdrew her consent owing to “personal reasons”. In addition, one interview was lost owing to human error, leaving baseline data for 37 (79%) women, collected during the third trimester of pregnancy. Methadone was used by 68.5 and 21.5% used buprenorphine. 27 The women had been in OMT on an average of 2.7 years prior to the third trimester interview. 12 Of the 37 women, 34 participated in the one year follow-up, but only information about those who participated in the four-year follow-up is included in this study. In the four-year follow-up, 26 women participated in the study.
Procedure
The study is one out of several on the cohort. Prior to conducting the four-year follow-up it was decided to extend the data collection with more variables, resulting in a need for a new approval from the regional ethics committee (REK). The approval was delayed and as a result we had to collect data on parts of this sample separately from the planned data collection.
When approval was obtained, participants also needed to provide an updated informed consent. Some consent forms were gathered by a researcher who met the mothers while they visited the cognitive developmental research unit at the University of Oslo. The mothers came with their four-year old children for various cognitive and social testing for another branch of the same project focusing on the children.30,32 All the mothers the researcher met with (n = 26), provided informed consent and participated in a scheduled interview.
The 10 mothers we did not get to meet personally were sent consent forms and reminders by postal mail. None responded. As the resulting dropout perfectly coincides with personal meeting versus postal contact, we believe it was due entirely to the type of contact and that the representativeness of the sample was not affected by this. One woman died from cancer before the four-year follow-up. This left 26 women (70%) of the women who joined the national cohort study during the third trimester, and 55% of the full national cohort. The mean age of the women at the four-year follow-up was 36 (range 27–48).
The proportion of women who reported substance use 30 days prior to the interviews during third trimester and/or the one-year follow-up was the same in the groups of women who did and did not participate in the four-year follow-up. This supports the assumption that dropout was because of procedure rather than more severe substance use.
Instruments
European addiction severity index (EuropASI)
The EuropASI is a semi-structured interview, widely used both for research and clinical purposes.33,34 It covers the following problem areas: substance use, employment and support status, family and social relationships, and physical, psychological, and legal issues. Previous studies have documented a satisfactory validity of EuropASI.34,35 Owing to criticism of the EuropASI composite scores,36,37 they were not used in our analyses; instead, data on substance use and psychological problems during the past 30 days and year prior to the interview is used.
Although we were not able to biochemically verify self-reported substance use in the follow-up, previous self-reports from this cohort showed that urine analyses and self-reported substance use were largely consistent,13,27 suggesting high reliability in self-reports in the sample.
In addition to EuropASI, the mothers were asked to provide additional information on the following three variables: (1) whether or not the child born just after they joined the study goes to kindergarten. (2) If child protective services had been involved in follow-up of the child they gave birth to four years ago. If so, provide information regarding type of support. The options were: preventive measures, voluntary measures, forced measures, and loss of custody. Preventive measures include parental counseling and support, child daycare, and respite care. Voluntary measures involve taking the child out of the parents care for a time limited period with the parents’ consent. In forced measures the child may be taken out of the parents care without the parents’ consent. Loss of custody means that the child will be living with other caregivers permanently. (3) If they had given birth to subsequent children after the child they were pregnant with when joining the study.
Statistics
Crosstab analyses with Fisher's exact test were used to examine whether there were significant changes in use of illegal substances, legal substances, and psychological problems from one to four years after the children were born. With a small sample size, P-level was set to 0.05. Descriptive information is presented as N (%). All analyses were conducted using IBM SPSS Statistics 21.0.
Results
Participant characteristics of women in OMT at four-year follow-up
The majority (92%) of the women were still in OMT four years after the children were born (Table 1). Around half (53%) lived with their child/children, but without a partner, and close to half (48%) were employed or studying. About one in four (24%) had given birth to other children after the child included in this study.
Background characteristics on women in OMT (n = 26) four years after the child was born.

Substance use at four-year follow-up
Use of illegal substances was low (4%), but a large proportion (39%) of the women reported using legal substances, mostly alcohol, during the 30 days prior to the interview (Table 2). Only one woman reported drinking to intoxication; the others reported only low alcohol consumption. There was no significant change in legal or illegal substance use from one to four years after the children were born.
Substance use during the last 30 days prior to baseline and follow-up interviews, among women in OMT (n = 26).

Data on substance use among women in OMT during third trimester and one year after was presented in Lund and colleagues. 12 To show development over time and to investigate if there was any change in legal or illegal substances from the one to the four-year follow-up, information on substance use at these data collection points was included in the table for the women who participated in the four-year follow-up.
There was no significant change from the one to the four-year follow-up.
Psychological and other problems related to substance use at four-year follow-up
Prevalence of psychological problems was high at the four-year follow-up, 69% reported one or more psychological problems (Table 3) which was significantly higher than 39% at the one-year follow-up (P = 0.009). The most common problems were problems concentrating, understanding, and/or remembering and almost half (46%) reported medical/somatic problems. None reported problems related to unemployment or legal issues/being involved in criminal activities.
Psychological and psychosocial problems during the last 30 days prior to baseline and follow-up interviews, among women in OMT (n = 26).

P = 0.009,.
Data on psychological problems among women in OMT during third trimester and one year after was presented in Lund and colleagues 15 ; to show development over time and to investigate change in psychological problems from one to four years after the children were born, information from these data collection points was included in the table for women who participated in the four-year follow-up.
Kindergarten attendance and child protection services involvement
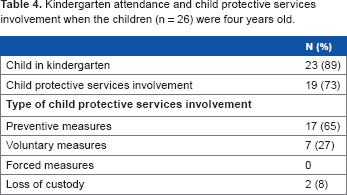
Most children (89%) attended kindergarten at age four (Table 4), and the child protective services were involved in 73% of the families. In most cases (65%) this was only with preventive measures, such as respite care.
Kindergarten attendance and child protective services involvement when the children (n = 26) were four years old.
Discussion
Knowledge about how mothers in OMT cope with substance use and related problems in the years following birth, is important to design policy which best supports them in this stage of life. The Norwegian setting offers a perspective on substance use and related problems over time in the absence of confounding factors that typically occur in this population, such as: poverty, homelessness and limited access to health care.
As during pregnancy and the one-year follow-up, illegal substance use remains low four years after the child was born. This finding may be explained by the fact that individuals who are stabilized on OMT are more stable, and less likely to relapse to illegal substance use. 38 This was the case for the women in this study, who had been in treatment for about two years before they got pregnant. 12 The “high control” setting in Norway may also have contributed to the low use of illegal substances.
Although there was no significant change in use of legal substances from the one-year to the four-year follow-up, the proportion of women who reported using legal substances was substantial. About a third of the women used alcohol; among these, only one woman reported drinking to the point of intoxication. The potential for adverse effects from combining alcohol and OMT gives reason to be extra cautious with alcohol consumption for this group. 39 According to the national guidelines for OMT in Norway, every patient should receive individualized treatment according to their perquisite. 40 Low alcohol consumption, such as drinking a glass of wine with dinner, may be unproblematic for some, but problematic for others. The issue should be addressed by the woman's support team on a case by case basis. The support team includes representatives from the specialist and regional health care, child protective services, and their medical doctor. 20
The proportion of women with psychological problems was significantly higher at the four-year follow-up, in line with what other studies on drug dependent women have found.10,11,41 Psychological problems can contribute to relapses if not treated. 10 It is therefore important that the women get professional help and take sufficient time to deal with their psychological issues.
Caring for young children can be stressful in itself for any mother; for those dealing with psychological problems it can be even more so,42,43 and leave little time to deal with their own psychological problems. This may have severe consequences for both mother and child. In the Norwegian setting, governmental support includes respite care and covering costs of kindergarten. The child protective services were involved in three quarters of the families when the children were four years old; mostly with preventive measures such as help with daycare, respite care, visiting homes, and parental guidance. In many cases, the mothers requested support from child protective services, and with 89% of the children attending kindergarten, this support contributes to them having time to deal with their own psychological issues. Depending on their situation this time is often also used for work or studies.
Mothers in OMT experience stigma and moralistic attitudes. Some politicians and health care personnel advocate that these women not be allowed to become pregnant and that being in OMT is incompatible with motherhood.3–5 This attitude can discourage opioid dependent women from seeking, or continuing OMT, which is considered the best available treatment for opioid dependence.1,44
Limitations and strengths
Dropout at two separate occasions could potentially be a problem. First, six women refused to participate at baseline, which prevents us from determining the extent they differ from the study participants. Second, there was concern for how representative the cohort was at the four-year follow-up. To control for this, we compared the level of substance use at previous data collection points between those who dropped out of the study to those who continued. We found no tendency to more serious substance use among women who dropped out. While all the women we met in person provided data, none of the women we did not meet participated. It is therefore reasonable to assume that dropout was related to procedure, rather than other factors. To our knowledge, this study is the first to follow mothers in OMT and their children over four years in a prospective study.
Conclusions
Our study shows that mothers in OMT cope well with substance use over time, given access to sufficient support, and in a high control setting. Many have psychological problems and time to deal with their own problems is important; in the Norwegian welfare setting most children of mothers in OMT attend kindergarten and the women are offered respite care allowing time to deal with these issues, attend studies or go to work. The findings suggest that a preventive governmental strategy with close support of mother and child, has a positive impact that contributes to making OMT and motherhood more compatible.
Author Contributions
Conceived and designed the experiments: IOL, HB, ER. Analyzed the data: IOL. Wrote the first draft of the manuscript: IOL. Contributed to the writing of the manuscript: IOL, HB, ER. Agree with manuscript results and conclusions: IOL, HB, ER. Jointly developed the structure and arguments for the paper: IOL, HB, ER. Made critical revisions and approved final version: IOL, HB, ER. All authors reviewed and approved of the final manuscript.
Disclosures and ETHICS
As a requirement of publication the authors have provided signed confirmation of their compliance with ethical and legal obligations including but not limited to compliance with ICMJE authorship and competing interests guidelines, that the article is neither under consideration for publication nor published elsewhere, of their compliance with legal and ethical guidelines concerning human and animal research participants (if applicable), and that permission has been obtained for reproduction of any copyrighted material. This article was subject to blind, independent, expert peer review. The reviewers reported no competing interests.
Footnotes
Acknowledgments
The authors thank the women for participating in the study. Thanks also to Gabrielle Welle-Strand, Monica Sarfi, and Brittelise Bakstad for invaluable support in this project, and Njål Andersen for English language editing and proof reading.