
Abstract
Background
Electronic cigarettes (ECs) are alternative-to-smoking nicotine delivery devices; consumers (commonly called vapers) use them in order to reduce or completely substitute smoking. The European Commission has released a proposal for a new Tobacco Product Directive that might reduce availability of nicotine-containing products, including ECs. In this study, the EC use patterns in subjects who have completely substituted smoking with EC use were examined by personal interviews. The study focused on nicotine levels used in order to achieve smoking cessation, reported benefits, associated side effects, and estimation of EC dependence compared with smoking.
Methods
Participants were 111 subjects who had completely substituted smoking with EC use for at least 1 month. Smoking abstinence was validated by measuring blood carboxyhemoglobin levels. Nicotine levels at initiation of EC use, at time of smoking cessation, and at time of interview were recorded. Dependence potential was assessed by asking the first question of the Fagerström Test for Cigarette Dependence (time until smoking the first cigarette and until first use of EC in the morning) and questions about perceived past dependence on tobacco cigarettes and present dependence on EC.
Results
Forty-two percent of participants reported quitting smoking during the first month of EC use. Liquids with nicotine concentration >15 mg/mL were used by 74% of users at initiation of EC use, while 16.2% had to increase the initial nicotine levels in order to achieve complete smoking abstinence. Seventy-two participants (64.9%) reported that from the time of smoking cessation to the time of the interview (8 months median duration of EC use) they reduced the nicotine concentration they were consuming; however, only 12% of the total sample was using ≤5 mg/mL nicotine concentration at the time of the interview. Side effects were mild and temporary. The vast majority of participants reported better exercise capacity and improved olfactory and gustatory senses. Perceived EC dependenct was significantly lower compared to smoking.
Conclusions
Nicotine levels appear to play an important role in achieving and maintaining smoking cessation in the group of motivated subjects studied. High nicotine-containing liquids were used while few mild and temporary side effects were reported. Proposals about regulation should consider the pragmatic use patterns of ECs, especially in consumers who have completely substituted smoking.
Introduction
Electronic cigarettes (ECs) have been marketed as smoking-alternative products that could be a part of tobacco harm reduction, a strategy of reducing adverse health effects by providing low-risk nicotine products to substitute smoking. 1 Awareness and use has significantly increased over the past few years 2 ; data from the International Tobacco Control Four-Country Survey showed that 2.9% of smokers were using ECs in 2010 and 2011, 3 while in the United Kingdom, 6.7% of daily smokers were using them in 2012. 4 They have caught the attention of public health authorities in recent years, and attempts to regulate them have been initiated. In several countries, such as Germany, Estonia, The Netherlands, and the United States, efforts to classify them as medicinal products were undertaken, but the courts decided against such regulations. 5
Recently, the European Commission released a proposal for a new Tobacco Product Directive (TPD) that introduces a new category of products called nicotine-containing products. 6 ECs are classified in this category and, according to the proposal, all EC liquids containing more than 4 mg/mL nicotine concentration should be banned unless they get approval as medicinal products. The nicotine threshold identified in this proposal was established by considering the nicotine content of medicinal products (nicotine replacement therapies, NRTs) for smoking cessation, which have already received a market authorization under the medicinal products’ legislation. 6 Recently, the proposal was altered, and the final TPD that will be submitted to the European Parliament states that all nicotine-containing ECs should be regulated as medicinal products.
NRTs, although better than placebo, have shown low long-term smoking cessation rates.7,8 A recently published meta-analysis found that 6 months sustained smoking abstinence is achieved by less than 7% of smokers. 7 The authors noted that, in most of the studies analyzed, regular behavioral support and monitoring was provided, making it unclear whether NRTs without additional support would be as effective. Sensory stimulation 9 and simulation of smoking behavior and cigarette manipulation 10 are important determinants of a product's effectiveness in reducing or completely substituting smoking; most of these features are absent in NRTs. On the contrary, ECs are unique in that they both mimic the rituals associated with smoking (hand-to-mouth movement, visible “smoke” exhaled) and provide sensory stimulation; therefore, they could be useful as smoking substitutes. However, nicotine delivery is equally important. 11 Studies using first generation EC devices found low nicotine delivery to and absorption by inexperienced users, even when using 16 mg/mL nicotine-concentration liquids.12,13 Despite that, anecdotal reports and small studies14,15 have shown that there is potential in reducing smoking. To understand this potential, it is important to evaluate how ECs are used by smokers who eventually manage to completely substitute smoking with them. Therefore, the purpose of this study was to examine the profile and EC use patterns in a specific group of exsmokers who have managed to completely substitute smoking with EC use without using any other aid. The study focused on evaluating nicotine levels used, reported side effects and benefits, and the dependency potential of EC compared with tobacco cigarettes.
Methods
Study Sample
Experienced EC users (commonly called vapers) aged 20 to 55 years participated in the study. The only inclusion criterion was that subjects should be former smokers who had completely substituted smoking with EC use for at least 1 month. Participants were recruited for research protocols evaluating the clinical effects of EC use, which were implemented in 2012 and early 2013. Subjects were included in the analysis irrespective of the type of EC devices or nicotine-level liquids they were using. Recruitment was made from visitors to the hospital where the study was performed and from an EC consumers’ internet forum in Greece where an announcement about the study was published. To make sure that participants did not smoke tobacco cigarettes, whole blood carboxyhemoglobin level was measured. If a level of more than 2% was measured,16,17 the participant was excluded from the analysis.
One hundred and thirteen vapers volunteered to participate (32 hospital visitors and 81 members of consumers’ Internet forum). Two subjects were excluded because of blood carboxyhemoglobin levels higher than 2%; the remaining 111 were interviewed by one of the researchers during a scheduled visit to the clinic to assess eligibility to participate in the clinical studies. None of the participants reported using any smoking cessation aid after starting using the EC or at the time of smoking cessation. Written informed consent was signed by all subjects before participating in the study. The protocol was approved by the ethics committee of our institution and conforms to the provisions of the Declaration of Helsinki. No financial or other compensation was provided to the participants.
Smoking History and ec use
Smoking history (smoking duration and cigarette consumption when participants were smokers) was recorded according to self-report. The Brinkman index was calculated as the product of years of smoking and number of cigarettes consumed daily. 18 Information about duration of smoking cessation and EC use, and daily consumption (in mL per day) and nicotine levels of EC liquids currently used was requested. To evaluate the nicotine concentration used in order to successfully substitute smoking, participants were asked to report (1) nicotine-concentration liquids used when they initiated EC use and (2) nicotine-concentration liquids used at the time they managed to quit smoking.
To assess past dependence on tobacco cigarettes, the first question of the Fagerström Test for Cigarette Dependence 19 was asked, “How soon after waking up did you smoke your first cigarette?” The answers were scored with 3 points assigned to “within 5 minutes,” 2 points to “between 6 and 30 minutes,” 1 point to “between 31 and 60 minutes,” and 0 points to “more than 60 minutes.” The same question was asked for EC use in the form, “How soon after waking up do you use the EC?” The same answer options and scoring system as that for smoking were applied. Two additional questions evaluating dependence were asked. The first was “How would you rate your past dependence on smoking?” And the second was “How would you rate your current dependence on EC use?” The answers were provided by using a 100-point visual analogue scale (VAS) line; the 0-point (left anchor) was “not dependent” and the 100-point (right anchor) was “extremely dependent.” A mouse-controlled cursor produced an X mark on the line at the point chosen by the participant. The score was automatically generated after pressing the “read out VAS value” button (www.vasgenerator.net). Questions were asked in random order at least 5 minutes apart during the interview in order to avoid any interaction between the 2 answers. Finally, open-ended questions were asked about perceived health benefits and side effects associated with the use of EC. All questions were asked verbally by one of the researchers during face-to-face interviews. The researcher recorded the answers provided by the participant. The only questions that were self-completed by the participants were the VAS questions.
Statistical Analysis
Kolmogorov-Smirnov tests were applied to check the normality of data distribution. Continuous variables were expressed as mean ± standard deviation (SD) or median (interquartile range [IQR]) and categorical variables as number (percentage). Wilcoxon signed ranks test was used to compare EC liquid nicotine concentrations at initiation of EC use, at smoking cessation, and at interview time. The same methodology was used to compare answers to questions evaluating dependence on tobacco cigarettes and EC. To evaluate the association between changes in nicotine concentration used and duration of smoking cessation, Kendall rank correlation coefficient (tau) was used. Additionally, logistic regression analysis was used to examine the association between duration of EC use and subsequent reduction in nicotine levels after adjusting for nicotine levels used to achieve complete smoking substitution; reduction in nicotine levels was the dependent categorical variable (no vs. yes). All P values reported are 2-tailed. Statistical significance was set at 0.05 and analyses were conducted using SPSS statistical software (version 18.0, SPSS Inc, Chicago, IL, USA).
Results and Discussion
Characteristics and Nicotine Levels used
The characteristics of the study group are displayed in Table 1. The majority of participants (84%) were males. A significant proportion of the study sample consisted of formerly heavy smokers (smoking more than 20 cigarettes per day). Forty-eight of them (42%) quit smoking during the first month of using ECs; 22 (19.8% of the whole group) quit on the first day. All participants achieved smoking abstinence by using second-generation (eGo-type batteries, 90.9%) or third-generation (variable voltage, often called “Mod”) devices (9.1%). Thirty-five participants (31.5%) reported that they initiated EC use with a first-generation cigarette-like device, They reported that these devices were only sufficient for reducing smoking consumption but not for smoking cessation. Importantly, 69 users (62.2%) mentioned that they unsuccessfully tried to quit smoking in the past, both without any aid (58.6% of the whole sample) and with the use of currently approved medical methods (30.6%).
Characteristics of electronic cigarette (EC) users.

Nicotine concentration of liquids used by the participants is shown in Figure 1. They all initiated EC use with liquids containing higher than 5 mg/mL nicotine; 74% of them used levels higher than 15 mg/mL. Eighteen participants (16.2%) reported that they had to increase the initial nicotine level in order to achieve complete substitution of smoking. Four of them increased nicotine levels from 18 to 24 mg/mL, 1 from 16 to 24 mg/mL, 1 from 12 to 24 mg/mL, 9 from 12 to 18 mg/mL, 2 from 9 to 18 mg/mL, and 1 from 6 to 12 mg/mL. No user decreased nicotine levels before smoking cessation. In total, 81% of EC users used liquids with higher than 15 mg/mL nicotine concentration in order to achieve complete substitution for smoking.
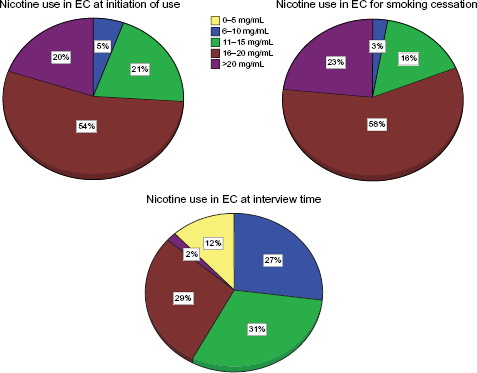
Nicotine concentration (mg/mL) used with the electronic cigarette (EC) at initiation of use, for smoking cessation, and at the time of the interview.
Nicotine concentration of the liquids used at the time of the interview was significantly lower compared with that used at initiation or at the time of smoking cessation (P < 0.001). Seventy-two participants (64.9%) reported that they reduced nicotine concentration compared with that used at the time of smoking cessation; however, only 5 users (4.5%) were consuming non-nicotine liquids at the time of the interview. Reduction in nicotine levels was statistically dependent on duration of smoking cessation (Kendall tau, 0.502, P < 0.001). After adjusting for nicotine levels used for smoking cessation, duration of EC use was significantly associated with reduction in nicotine concentration (logistic regression analysis: B = 0.364, P < 0.001).
Side Effects and ec Dependence potential
Side effects were mostly temporary and mild. Thirty participants (27%) reported throat irritation that resolved completely in 28 participants and partially in the rest. Cough appeared in 15 participants (13.5%) and was completely resolved shortly after initiation of EC use. Eight participants (7.2%) reported gastrointestinal discomfort or epigastric burning pain, while six participants (5.4%) reported palpitations, which resolved spontaneously. Other side effects reported by less than 5% of participants were headaches, sleepiness or sleeplessness, atypical chest pain, and gum and nose bleeding. There were no reports of allergic reactions. Interestingly, the majority of participants (79 users, 71.2%) reported weight gain after initiating EC use. No subject reported seeking medical attention or having long-term health implications. On the contrary, most of them reported improved exercise capacity (76.6%) and improved olfactory and gustatory senses (81.9%). Other reported benefits included less morning cough (58.6%) and better sleep (22.3%).
By evaluating and comparing answers to questions about tobacco cigarette and EC dependence, significant differences emerged. In particular, the median (IQR) score for the question “How soon after waking up did you smoke your first cigarette?” was 2 (2–3), while for the respective question for EC use it was 2 (1–2). Moreover, the median (IQR) score of the 100-point visual analogue scale question about cigarette dependence was 83 (77–89), while for EC dependence it was 59 (49–66). EC dependence was significantly lower for both questions (Wilcoxon signed rank test, P < 0.001).
Discussion
This study specifically focused on vapers who had completely substituted smoking with EC use. Liquids with high levels of nicotine were used in order to achieve smoking abstinence. EC use appeared safe, with few and mild side effects reported by the group studied; in most cases side effects were not necessarily linked with the level of nicotine used. In addition, a gradual decline in nicotine concentration use was observed as well as longer time until first use of EC in the morning compared with previous tobacco smoking was reported.
ECs are devices with unique features compared to any other product in tobacco harm reduction. They deliver nicotine, thus dealing with the chemical part of the addiction, and, at the same time, they provide sensory and motor stimuli similar to smoking. Although both characteristics have been the subject of criticism (ie, delivery of an addictive substance and normalization of smoking behavior), they are probably the most important reasons for ECs’ increase in awareness and use; 20 additionally, much of their probable success in reducing cigarette consumption should be attributed to these features. Anecdotal reports, communication with users, surveys and a nonrandomized pilot study provide important evidence for their effects as smoking substitutes,14,15,21 while a recent randomized double-blind study showed that they can be effective in smoking reduction and cessation. 22 In this context, it is important to examine the behavior and patterns of EC use in exsmokers who have reported complete substitution of smoking with EC use. This study focused on such users and provides information about the patterns of EC use in order to achieve complete substitution of smoking. Smoking abstinence was objectively assessed by measuring whole blood carboxyhemoglobin levels in all participants.
More than 80% of vapers from this sample quit smoking cigarettes by using EC liquids with nicotine levels higher than 15 mg/mL. It could be argued that their choice was based on advice they received from sellers or over the Internet about the levels of nicotine needed at initiation of EC use. However, we noted that 16.2% of participants had to increase the level of nicotine in order to achieve complete smoking substitution. This supports the assumption that high levels of nicotine are probably necessary in order to achieve smoking abstinence. The reason for using such high levels could be the lower potential for nicotine absorption from EC use, which has been supported by clinical studies.12,13 However, in these studies, smokers who were using the EC for the first time were evaluated and first generation (cigarette-like) ECs were used. It has been observed that ECs are used less intensively by novice users, 23 and participants in this study reported that first generation devices could reduce cigarette consumption but were not very efficient as complete smoking substitutes. A recently published survey of vapers found that exsmokers were more likely to use second or third generation devices compared with current smokers, supporting the concept of higher effectiveness of modern devices. 24 Such devices have higher-capacity batteries, allowing the consumer to use them for more time before being discharged, with some of them having the ability to deliver higher energy to the resistance and wick. Additionally, atomizers store more liquid and give the possibility to refill them with a variety of flavored liquids instead of having to use prefilled cartomizers. However, even the small cigarette-like devices are evolving, and new models may be more efficient compared with those available few years ago. 22 Finally, a recent study found that high levels of nicotine concentration are needed in order to deliver nicotine amounts similar to tobacco cigarettes, since the evaporation rate in ECs is slow. 23 Despite that, the majority of participants in our study reported weight gain during the initial period of EC use. Since one of the effects of nicotine is elevated metabolic rate, and smoking cessation results in weight gain,25,26 it is reasonable to assume that use of second-generation devices may also not result in blood nicotine levels similar to using tobacco cigarettes, at least in some users; alternatively, it could be attributed to the lack of experience during the initial period of EC use. A small study found that experienced vapers had significantly elevated blood nicotine levels after using modern EC devices. 27 More studies are needed in order to compare the nicotine delivery potential between different devices.
Recently, ECs have been the focus of regulatory efforts by the European Union. The released proposal for a new TPD initially dictated the ban of liquids with higher than 4 mg/mL nicotine concentration unless they are approved as medicinal products, 6 while the final decision implemented the medicinal regulation for all nicotine-containing liquids (irrespective of the nicotine concentration). The reasons for such regulation focus on consumer safety and precise nicotine (and other ingredients) labeling, similar to regulations applied to NRTs. However, the main differences between NRTs and ECs are that the latter provide pleasure to the user, 28 address the bio-behavioral aspect of smoking addiction, 29 and have an additional social aspect. 28 ECs are marketed and used as smoking substitutes; therefore, in terms of marketing competition, they are mainly competing with tobacco cigarettes. 30 Medicinal regulation could reduce technological evolution and development of more efficient products because the cost would be too high to get approval for new products that are developed at a fast rate; this would inevitably restrict the variability of devices and liquids available for consumers. In this study, participants were predominantly using modern devices in order to achieve and maintain smoking abstinence. Procedures like having to get a doctor's prescription in order to buy ECs could also discourage smokers from trying ECs, since they are already more complex in their use compared to tobacco, and such procedures would additionally make them less easily accesible to buy. It would also be impractical for current EC users, since observations from this study and from surveys indicate that they are mostly used as long-term substitutes for smoking rather than as a smoking-cessation method used for a short period; thus, vapers would have to follow such procedures for a long time.
Participants in this study used liquids with high levels of nicotine in order to achieve complete smoking abstinence. They reported few side effects, which were mostly temporary; no subject reported any sustained adverse health implications or needed medical treatment. Several of the side effects may not be attributed to nicotine. In addition, almost every vaper reported significant benefits from switching to the EC. These observations are consistent with findings of Internet surveys21,24 and are supported by studies showing that nicotine is not cytotoxic, 31 is not classified as a carcinogen, and has minimal effects on the initiation or propagation of atherosclerosis. 32 It should be mentioned that participants in this study and in surveys are mostly motivated users; thus, it is expected that such a population has a positive experience from using ECs. During the period after smoking cessation, a significant proportion of participants managed to decrease nicotine levels, and they reported lower dependence on EC compared with smoking. However, only 12% were using liquids with ≤5 mg/mL nicotine concentration (4.5% were using non-nicotine liquids), suggesting that nicotine may be an essential part of EC use, even for users who have achieved complete smoking abstinence for several months. In fact, the definition of tobacco harm reduction is to reduce the burden of disease without eliminating nicotine use, 33 and ECs should be considered part of this strategy. Therefore, any decisions by public health authorities should ensure that availability of nicotine-containing liquid is not restricted; otherwise, the possibility of smoking relapse in this population cannot be excluded. This could have significant adverse health implications, since smoking is a significant risk factor for a variety of diseases34,35 and can produce sub-clinical disease at an early age. 36 Obviously, product safety and quality should be ensured, and monitoring of long-term use should be implemented; however, there are standard consumer protection regulations that could be applied without the need for strict and inflexible medicinal regulation. 30
Some limitations apply to this study. We examined a convenience sample of vapers willing to participate to clinical studies. The subjects were probably more motivated than those found in the general population. The purpose of the study was not to evaluate the potential of the EC as a smoking cessation tool, but to examine the patterns of use and the experience of exsmokers who had successfully substituted smoking with EC use. Although motivation is unlikely to play a role in the selection of nicotine levels used for smoking cessation, it is expected that such a group may have experienced greater benefits and fewer side effects from EC use compared with a randomly selected sample. The majority of participants in this study were males. This is consistent with observations from Internet surveys.15,24 Reasons for this could be that ECs are less appealing or less successful in females as smoking substitutes. However, this should be addressed in a randomized study before making any definite conclusions. Dependence on smoking was reported retrospectively in this study and may not be accurate; additionally, only the first question of the Fagerström Test for Cigarette Dependence was asked. However, this is a key question in the dependence test 37 and asking more questions would potentially increase bias due to the retrospective nature of the answers concerning smoking. Moreover, the gradual reduction of nicotine levels reported by 64.9% of users supports the assumption of reduced potential for dependence; this is in agreement with a recent study reporting lower abuse potential for ECs compared with smoking. 38
Conclusions
In conclusion, high nicotine-containing liquids are probably essential for initiating and maintaining smoking abstinence in a group of motivated vapers. Although less dependence was reported relative to smoking, prevalence of nicotine use was high even after several months of EC use. Public health authorities should consider the evidence from this and other studies that ECs are used as long-term substitutes to smoking by motivated exsmokers and should adjust their regulatory decisions in a way that would not restrict the availability of nicotine-containing liquids for this population.
Author Contributions
Conceived and designed the experiments: KF. Analyzed the data: KF, GR, DT, SK. Wrote the first draft of the manuscript: KF. Contributed to the writing of the manuscript: SK, VV Agree with manuscript results and conclusions: KF, GR, DT, SK, VV. Jointly developed the structure and arguments for the paper: KF, GR. Made critical revisions and approved final version: DT, VV. All authors reviewed and approved of the final manuscript.
Funding
Author(s) disclose no funding sources.
Competing Interests
Author(s) disclose no potential conflicts of interest.
Disclosures and Ethics
As a requirement of publication the authors have provided signed confirmation of their compliance with ethical and legal obligations including but not limited to compliance with ICMJE authorship and competing interests guidelines, that the article is neither under consideration for publication nor published elsewhere, of their compliance with legal and ethical guidelines concerning human and animal research participants (if applicable), and that permission has been obtained for reproduction of any copyrighted material. This article was subject to blind, independent, expert peer review. The reviewers reported no competing interests.