
Abstract
Objective
The purpose of this study was to compare the therapeutic effects of portable and stationary tractions on treatment outcomes in patients with mechanical neck disorders (MNDs).
Methods
Forty-one participants with MNDs were randomly assigned to either portable traction or stationary traction. Participants' pain level, activity limitation, disability, and neck range of motion were measured before and after 6 weeks of intervention. Inferential statistics for comparing the treatment outcome involved paired t-test and two-way analysis of variance at P < 0.05.
Results
The mean age of participants was 47.3 ± 10.5 years. After intervention, there were significant improvements in both groups. However, the portable traction group had significantly higher score on neck flexion than the stationary traction group at baseline (portable: 27.1 ± 6.0, stationary: 22.1 ± 6.8; P = 0.009) and after intervention (F-ratio = 15.0; P = 0.001).
Conclusion
Inclusion of both portable and stationary tractions to usual physiotherapy provided comparable treatment outcomes in patients with MNDs.
Introduction
Neck pain is a commonly reported musculoskeletal disorder that is usually accompanied by appalling measures of socioeconomic burden on the sufferers. 1 Activity-related neck pain is a prominent symptom of most mechanical neck disorders (MNDs), which include whiplash-associated disorders, torticollis, myofascial neck pain, cervical spondylosis, and radiculopathy.2,3 It is characterized by insidious onset, which could originate from multiple factors such as poor posture, anxiety, depression, and muscle strain arising from participation in sports, occupational antecedents, and degenerative changes. 4 MNDs are more common during middle age, with females recording higher prevalence than males. 5 These could lead to high degree of morbidity and restricts patients' participation in various activities of daily living. 6 Efforts geared toward determining the most effective means of managing the disorders are therefore paramount and could help in selecting appropriate interventions in clinical practice.
Mechanical cervical traction is part of the usual intervention used by practitioners of orthopedics and physical therapy in the management of patients with neck pain.7,8 Cervical traction, among other conservative modalities, is often prescribed as adjunct to usual physiotherapy, such as manual therapy, heat therapy, and electrophysical agents. Usually, traction is administered in the hospital setting, thereby requiring frequent visits by patients. In Ghana, most physiotherapy facilities are equipped with stationary traction device, which often compels patients to visit these facilities to receive treatment. This mode of care has serious indirect health care cost implication for patients and their families.
In many developing countries including Ghana, physiotherapy services are still unavailable in primary care settings, making accessibility a serious challenge to many patients. One way to curtail the incessant deprivation of health care needs among people in poorly resourced settings is the effective use of a patient-centered approach, in which clients become active members of the management team. In the United Kingdom, patient self-management is applied for most musculoskeletal conditions to curb issues arising from availability, accessibility, and cost. 9 Although the availability of various portable mechanical and electrical therapeutic devices in developing countries is beginning to drive the health care service toward this trend, the outcome of treatment on the end users has not been sufficiently documented.
Portable traction could serve as a potential option to stationary traction, with added advantage as regards cost-effective health care approach. The treatment frequency varies greatly and could range from once to thrice weekly or even several times daily with treatment duration of about 30 minutes. 10 The present study was designed to compare the therapeutic effects of portable and stationary cervical tractions in the management of MNDs with regard to self-reported pain, activity limitation, disability, and the neck's range of motion. We hypothesized that the treatment outcome of portable traction will not be significantly different from that of stationary traction after 6 weeks of intervention.
Participants and Methods
Study Design
A quasi-randomized clinical trial was adopted in this study. Participants were randomly assigned to two parallel groups simultaneously to determine whether the application of portable cervical traction would replicate the same efficacy as found in the stationary traction device. The protocol adopted in this study is in conformity with the principles of the Declaration of Helsinki for human research.
Participants
Forty-one patients with MNDs were enrolled from the outpatient physiotherapy departments of Korle-Bu Teaching Hospital, 37 Military Hospital, and Tema General Hospital in Greater Accra Region, Ghana. Inclusion criteria were as follows: diagnosis of MNDs arising from cervical spondylosis, whiplash, and myofascial pain; age between 20 and 65 years; and absence of medical complaints such as dizziness. Patients with history of metallic implants in the cervical region, spinal fracture or previous spinal surgery in the neck, osteoporosis, and acute strain or sprain with ongoing inflammation were excluded.
Randomization
Participants were randomly assigned to two groups by an independent person. Randomization was done through balloting (Fig. 1). The portable traction group consisted of 21 participants (n = 21) compared to 20 participants in the stationary traction group (n = 20). Although patients were blinded to treatment allocation, they were duly informed about receiving traction therapy. Three physiotherapists working in the selected sites participated in this study. A prestudy meeting was organized by the researchers to discuss the purpose of the study, measurements, intervention, and ethics. The participating physiotherapists administered treatments but were not blinded to treatment allocation. They were, however, excluded from taking part in measurement of treatment outcomes.
Flow diagram of the recruiting process.
Apparatus and Instrumentation
An electrical cervical traction device with four-sided control panel was used as stationary mechanical traction. The portable cervical traction device used in this study was the Folee Neck traction (J008-B). It adopts flocking cloth of soft stockinette with incorporation of tensile elasticity, which is connected to a latex ball through a long latex tube for pressure regulation. The Neck Pain and Disability Scale (NPAD) is a 20-item scale that measures neck movement, neck pain intensity, neck pain on emotions and cognition, and the degree to which the pain interferes with activities of daily living. 11 Patients respond to each item by marking along a 10-cm line the characteristics of a visual analog scale. The score of each item ranges from zero to five, and the total is 0-100, where 0 means no pain and 100 means maximum pain. 11 The Patient Assessment Scale (PAS), on the other hand, is a 13-item scale with two 10 cm lines representing the visual analog scales. It measures the activity level of patients by assessing the global and local effect of pain as well as the functioning of the patient. The first ten questions have a score range of 0 to 3, where 0 means the ability to perform activity without any difficulty and 3 means inability to perform activity. The total score for the 10 questions is converted using a special scale in the assessment form. Scores for the last three questions range from 0 to 3.3, with an increasing score representing difficulty in performance of activity. The total score is obtained by the summation of the converted score and the score obtained from the last three questions. A greater score is indicative of the higher level of difficulty in performing activities of daily living. Weighing scale and double-armed goniometer were also used to measure the body weight and neck flexibility of the participants, respectively.
Procedure for Data Collection
Approval for the protocols of this study was obtained from the Protocol and Ethics Review Committee of the School of Allied Health Sciences, University of Ghana (Ref. SAHS ET./10341649/ AA/1A2013-2014). Participants were briefed about the aims and objectives of the study, after which all consented to participate. They all signed an informed consent form before the commencement of the study.
Measurements
Demographic data such as participants' age and gender were collected. Before intervention, baseline scores for activity-related pain, disability, activity limitation, activities of daily living, and neck range of motion were determined using NPAD, PAS, and double-armed goniometer. In addition, each participant's body weight was measured to determine the amount of traction force required to set the stationary traction device. The force was determined as 10%-15% of the participant's body weight. 12
Treatments
The usual care physiotherapy approaches in this protocol were mainly superficial heat therapy and therapeutic exercises that included stretching of paraspinal soft tissues, as well as contract-relax, hold-relax, and free active exercises. These techniques were standardized among the physiotherapists across the two groups. Traction was administered after the usual care had been given for both groups as follows.
Portable Cervical Traction (Group 1)
Participants sat comfortably on a chair with armrest and the stockinette of the traction was anchored around their necks. The stockinette was adjusted according to the size of the patient's neck using the attached Velcro strap. The steel screw was tightened, while the latex ball was pumped to inflate the stockinette to a moderate pressure that was tolerable and comfortable. This was determined by feedbacks provided by patients. Patients had a daily traction treatment for 20 minutes.
Stationary Cervical Traction (Group 2)
Patients were similarly instructed to sit on a chair with armrest, which was positioned under a pulley system and a two-padded canvas headpiece was applied to the neck. One pad was placed beneath the anterior part of the mandible and the other beneath the occiput posteriorly. The canvas served as the anchor through which traction force was applied to the neck. Traction force of 10%-15% of the patient's body weight and treatment duration of 20 minutes were selected on the control panel for each session of treatment. Patients were given safety instructions, including warning signs to terminate treatment in the event of untoward feeling.
Reassessment
Evaluation of the treatment variables was repeated at the sixth week of the intervention for both groups by an independent assessor who was blinded to the assignment of the patients.
Data Analysis
Data analysis was performed with intention-to-treat principle using SPSS (version 20.0). Descriptive statistics of mean, standard deviation, and percentage were used to summarize sociodemographic data and clinical attributes of patients. The effects of continuous outcomes (means with 95% confidence intervals) were expressed between baseline and week 6. Comparison of pre- and postintervention outcomes within each group was determined using paired t-test, while mixed-design two-way analysis of variance was used to determine the difference between the two groups on the selected variables. A P-value of 0.05 (two-tailed) was set as the level of significance.
Results
Comparison of baseline parameters of participants.

Significance at P < 0.05.
Treatment Outcome on Primary and Secondary Measures within Groups
Two-sample paired t-test for within-group comparison on primary measures.
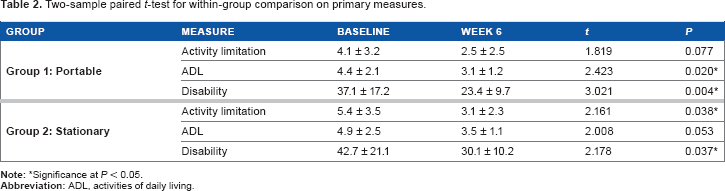
*Significance at P < 0.05.
Two-sample paired t-test for within-group comparison on secondary measures.

Significance at P < 0.05.
Comparison of Treatment Outcome between Groups on the Primary and Secondary Measures
Two-way analysis of variance for between-group comparison of portable and stationary tractions on primary measures.
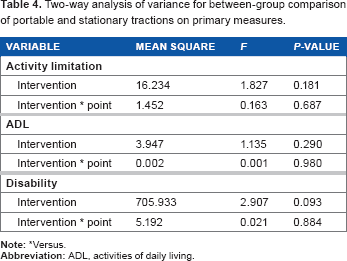
Versus.
Two-way analysis of variance for between-group comparison of portable and stationary tractions on secondary measures.

Versus.
Discussion
In a developing country like Ghana, issues arising from accessibility and affordability of health care services have justified the need for a patient-centered management approach such that patients with musculoskeletal disorders can become actively involved in tackling their health issues while reducing facility-based care. The present study thus compared treatment outcomes of patients with MNDs who received usual physiotherapy care in addition to either portable traction or stationary mechanical traction. The overall outcome of this study showed marked improvement in the participants following the application of either of the two devices combined with other management techniques. We therefore accept our initial hypothesis, which suggests that the treatment outcome of portable traction will not be significantly different from that of stationary traction after 6 weeks of intervention.
The results of this study showed significant improvements for both groups on pain intensity, activities of daily living, disability level, and neck range of motion. These findings justify the use of portable mechanical traction as a potent substitute for stationary mechanical traction in clinical practice. Our findings are consistent with the report of Moeti and Marchetti, 13 who reported reduction in pain and disability in their subjects following cervical traction application. According to these authors, pain experienced by patients with neck disorders affect their performance of activities of daily living and disability levels. Therefore, reduction in pain levels presupposes reduction in disability levels and increased performance of daily activities.
Conventionally, alleviation of clinical deficits with the use of traction is owed to the stimulation of large afferent A-beta pain fibers, which reduces pain intensity presynaptically at the spinal level. Increase in neck flexibility, on the other hand, may be attributed to decrease in muscle spasm and increased blood circulation to affected areas, thereby contributing to the healing process and hence their ability to move the neck better. 14 In addition, there is stretching of paravertebral muscles of the neck region when a traction force is applied, resulting in reduced muscle tension and spasms.15,16 Participants who received portable traction are believed to derive their therapeutic gains through these biomechanical and physiological features. Participants in both portable and stationary mechanical tractions were not significantly different on all the outcome measures. The apparent better neck flexion among the patients in the portable neck traction group is due to the baseline difference with their counterparts who received stationary traction and not necessarily a sign of superiority over the latter.
This finding has clinical implication for physiotherapists and orthopedic physicians with regard to a patient-centered and cost-effective approach in practice. In view of the disproportionate ratio of patients to physiotherapists in Ghana, household therapeutic modalities such as portable traction can be prescribed in addition to patients' home program with a view to get clients involved in their health management.
Limitations
Our study has potential limitations. The primary limitation could be attributable to the lack of a control group. Even though this was not applicable in our adopted design, a study design with the inclusion of a control group is often considered stronger. Addition of a control group is therefore highly recommended for consideration in future trials.
Additionally, our sample size was small (41 participants), thereby necessitating caution in generalizing the findings of this study. Studies with small sample sizes are often characterized by weak statistical power. In connection with this, the treatment protocol lasted 6 weeks in this study. The short duration, occasioned by decline in compliance of the clients due to various reasons, has made it impossible to extrapolate the usability of portable traction on a long-term basis from our findings. Lastly, the duration of patients' symptoms was assessed but not documented for statistical analysis, which also created a loophole with regard to the objective “effect size” obtained with both interventions.
Within the above-mentioned limitations however, the study has been able to suggest that both portable and stationary tractions may be beneficial to patients with MNDs. However, further studies with large sample sizes are needed to confirm these findings.
Conclusion
On the basis of the findings from this study, it can be deduced that portable and stationary traction devices are equally effective in the management of MNDs. It thus suggests that mechanical traction (either portable or stationary) yields significant improvement in patients with MNDs when combined with other conservative treatment techniques. Prescription of portable tractions for patients with MNDs is therefore justifiable, particularly in underresourced physiotherapy facilities. These findings can serve as a platform for its endorsement in primary care settings wherein fully equipped physiotherapy setups are lacking.
Author Contributions
Conceived and designed the experiments: AIB. Analyzed the data: AIB and EB. Wrote the first draft of the manuscript: AIB. Contributed to the writing of the manuscript: EB, JAC. Agree with manuscript results and conclusions: EB, JAC. Jointly developed the structure and arguments for the paper: AIB, EB, and JAC. Made critical revisions and approved final version: AIB, EB. All authors reviewed and approved of the final manuscript.
Footnotes
Acknowledgment
We acknowledge the kind gesture of the Managing Director of CIVARC, Limited, Nigeria, for the provision of some portable cervical traction devices used in this study.