
Abstract
Stuttering is a complex communication disorder that impedes the normal flow and pattern of speech, which is characterized by involuntary audible or inaudible pause, repetitions, prolongations, blocks, etc. Other than the core behaviors, people who stutter experience various other problems such as fear, anxiety, depression, shame, etc., which can in turn affect the quality of life (QOL). The purpose of this study is to develop a questionnaire in order to assess the QOL of people who stutter. A total of 30 participants aged between 18 and 30 years were enrolled for the study. Out of the stutterers included, 15 were employed and 15 were non-employed/students. The study was carried out in two phases. The first phase involved the development of a questionnaire based on literature search and available tests. The second phase involved administering the validated questionnaire on the participants. The questionnaire consisted of six domains targeting (1) speech-related fear and anxiety, (2) interpersonal and social relationships, (3) behavioral reaction to stuttering, (4) educational status, (5) employment and job opportunity, and (6) effect of speech therapy. For each item, response scales were organized (2—almost always, 1—sometime, 0—not at all). Developed questionnaire showed good content validity for all the domains and questions. The result of Cronbach's alpha for each domain indicates moderate internal consistency and excellent internal consistency for the overall questionnaire. Multiple domains were observed to be affected among adults who stutter, and the differences were not found to be significantly different as compared to the available QOL data from other cultural settings.
Introduction
Stuttering is one of the communication disorders affecting the fluency of speech that results in the disruption of speech. The onset of stuttering is mainly seen during the developmental period of a child's communication skills, most commonly between the ages of two to five years. This is called developmental stuttering. 1 The incidence of stuttering reported in the literature is higher in males than females with a ratio ranging from as low as 2.3:1 2 to as high as 5:1. 1
Stuttering can occur because of various factors such as genetic, neurogenic, stress induced, and environmental, but the exact cause of stuttering is unknown. The most obvious characteristics of stuttering are abnormal disfluencies, which result in stoppage of the forward flow of speech. Some disfluencies are normal in speech during conversation, but the speech of adults who stutter generally contains stuttering-like disfluencies, which include repetitions, prolongations, blocks, and pauses.3,4 To add on to the disfluent moments, adults who stutter may show different physical behaviors, and these behaviors are called secondary behaviors. Secondary behaviors are usually seen simultaneously with the stuttering events. The associated physical features include jerking of the head, eye blinks, lips or face tremors, tremors of muscles, abnormal breathing movements, movement of legs, and fist clenching. Adults who stutter experience many problems other than speech-related difficulties. The person's negative emotion toward stuttering often adds a great deal of complexity to the disorder. 3 Many adults who stutter report that they experience negative emotions and cognitive reactions associated with their communication difficulties, such as anxiety, fear, helplessness, anger, guilt, embarrassment, and frustration, with limitations in the person's social, occupational, and educational experiences.5,6 These specific types of feelings not only have an impact on the person's ability to effectively communicate but also affect the overall well-being of the individual. Most of the treatment outcomes follow the trend of understanding the disorder by its observable characteristics and give importance to improving fluency of speech. It is also important to target feelings and attitudes of adults who stutter because adults who stutter report that they experience negative reactions to stuttering, have difficulties in speaking in different circumstances because of fear and anxiety, and have difficulties in achieving their goals in life. Research reports five similar characteristics of adults who stutter. 7 The first characteristic is that they avoid conversation in many situations because of fear of being laughed at by others or misunderstood. Adults who stutter are shy and often withdraw from social gatherings. The second characteristic commonly seen in many adults who stutter is an inability to express their anger in an open way, owing to fear. The third characteristic is that they experience depression. Depression may be because of the fluency disorder. The fourth characteristic is guilt, the feeling that they could stop stuttering if they had more self-control. The fifth characteristic is anxiety, which is one of the problems that adults who stutter usually report. Anxiety about speaking can come from anticipating negative reaction from family members, friends, and other listeners. There are also other studies that have reported the presence of similar experiences among adults who stutter.8–11
Owing to these behaviors and their associated characteristics, stuttering may negatively impact their lives, with each disfluency being a fearful and anxiety-filled experience. Furthermore, adults who stutter are nervous and tensed while speaking. Various difficult experiences can affect a person's day-to-day life, personality, and personal and social relationships. Stuttering affects relationship with family and with friends as well. Moreover, family's and friends' reactions and attitude about stuttering can have a greater impact on the people who stutter. The impact of stuttering on one's life has been described in terms of impairment, disability, and handicap. 12 The impairment of stuttering is the physical or psychological factors that lead to stuttering behaviors (eg, speech disruptions). When stuttering leads to activity limitations, it can be viewed as a disability. Finally, stuttering can become a handicap if it limits the individual from fulfilling everyday needs, including education, employment, and social needs. There has been a realization of the need for research on the outcomes of stuttering that will help in understanding the disorder in its totality so that more specific intervention plans can be made. Quality of life (QOL) measures provide those aspects that formal tests do not assess.
QOL is defined as a person's perception of his/her position in life in the context of the culture and value systems in which he/she lives, and in relation to his/her goals, expectations, standards, and concerns. 13 QOL is a broad concept, which includes the person's independence level, psychological state, physical health, and social and family relationships.
Factors determining QOL is classified into four categories that include global, external, interpersonal, and personal domains. 14 These can be used to assess the quality of an individual and a social group. Global domain evaluates macro environment, human rights, and politics. External domain evaluates work, standard of living, and housing. Interpersonal domain evaluates relationship with parents, family, and friends. Personal domain evaluates physical, psychological or emotional, and spiritual statuses.
Main aspects affecting QOL recognized in numerous fields of science include the following factors: physical well-being, material well-being, and social well-being. Physical well-being includes factors such as health and functional states, independence, work, and personal safety. 15 Studies have put forward a broader understanding of physical well-being and supplement health aspects with rest, leisure, hobbies, and entertainment, which define an individual's ability to perform daily tasks. 16 From the financial viewpoint, another factor affecting QOL is material well-being. Material well-being includes factors such as an economic state (income), housing/living conditions, and occupation.15,17,18 Social well-being is perhaps the major group of factors affecting QOL. Social well-being includes family, leisure, and social life.
QOL can be assessed in many ways such as by interviewing the patient and family members, by conducting a health survey, by administering different tests, and by administering a QOL questionnaire. There are several generic QOL questionnaires and also disease-specific QOL questionnaires. These questionnaires give information about the individual's overall well-being or comfort and also about the health-related condition.
QOL measures have currently been an important aspect both in terms of clinical management and in terms of research in fields of science. Currently, there has been increased emphasis on documentation of different aspects such as functional outcomes, variations in emotional responses, and QOL for a wide range of disorders.19–21 There are a number of instruments available for assessing the comprehensive aspects of stuttering, such as the Speech Situation Checklist, which delivers information about a speaker's speech-related anxiety in different speaking conditions; 22 the Self-Efficacy scale for adults who stutter, 23 which provides information about a person's self-confidence about maintenance of fluency in different speaking situations; the Subjective Screening of Stuttering severity, 24 which observes the speaker's self-rated stuttering severity, external or internal locus of control, and avoidance of situations or words; and the Overall Assessment of the Speaker's Experience of Stuttering (OASES), 25 which is a self-rating questionnaire to assess the speaker's overall views about stuttering, emotional, behavioral, and cognitive reactions to stuttering, efficient communication difficulties, and QOL.
Apart from various factors discussed here, the determination of the QOL of an individual significantly depends upon the cultural background, which includes a set of values, standards, customs, and traditions associated with a particular society. Culture consists primarily of the symbolic, ideational, and intangible aspects of human societies. Culture is not artifacts, tools, or other tangible elements but how the members of the group interpret, use, and perceive them. It is the values, symbols, interpretations, and perspectives that distinguish one people from another in modernized societies. 26 The communication styles have been reported to get affected by the multicultural factors. These styles are major factors to be considered during the assessment process. These include rules for eye contact, proxemics, silence, laughter as a communication device, appropriate topics of communication, when and how to interrupt, and use of humor. 27 Many researchers have emphasized the need to adopt a culturally sensitive approach with respect to stuttering.28,29 There may be negative attitudes toward adults who stutter within their own cultures. 30 Factors such as degree of exposure to stuttering, education, and amount of direct contact have been found to affect perceptions of adults who stutter within their cultures. 31 Several investigations have examined the influence of culture on stuttering development.32–35 Nevertheless, stuttering has an impact on identity, the QOL of culturally and linguistically diverse populations.31,33,36–38 There are reports discussing the QOL of adults who stutter in different cultural settings. 39 The literature in sociology describes Indians to follow a high culture communication style. The communication style of Indians has been reported to be poetic, including elegant and imposing forms of speech. It is very polite, with expressions of humility and honorific and respect terminologies. 40 Recently, there is a drastic shift observed in the Indian culture because of technology, trade, travel, and television. 41 A recent study comparing Indian communication styles to those observed in the West reported Indians to possess more dramatic style of communication. 42 Indian culture has been observed to be one of the oldest and is immensely diverse with many distinct pursuits, vastly disparate convictions, widely divergent customs, and a veritable feast of viewpoints. 43 Indian society is a hierarchical system where all obligations and duties arise from multiple positions such as being a family member, a member of a work group, an employee, or an employer. 44 Therefore, the diversity and differences in Indian culture and communication styles may pose a different impact on QOL of adults who stutter because speech is the most important mode of communication. However, there is a dearth of literature exploring QOL of adults who stutter in Indian scenario.
Method
The focus of this study was to assess the QOL of adults who stutter in Indian population. This study was conducted at a multispecialty hospital at Mangalore, Karnataka, India. The study followed a cross-sectional study design with convenient sampling. The ethical approval was obtained for the study from Institutional Ethical Committee Board prior to the conduction of the study, and the research complied with the principles of the Declaration of Helsinki. A formal consent was obtained from all the participants of the present study before including them in the study.
Participants
A total of 30 participants aged between 18 and 30 years were enrolled in the study. All the participants were diagnosed with mild-to-moderate degree of stuttering as per the standard operating protocol for the assessment of stuttering followed at the Department of Audiology and Speech Language Pathology of the hospital. The protocol relies on the Stuttering Severity Instrument-3 45 and the perceptual judgment of the qualified professional. All the participants were attending therapy for more than six months. The individuals above 18 years of age, diagnosed with stuttering based on Stuttering Severity Instrument, with minimum schooling of 10th standard and above, and those possessing the ability to read and write in English were included in the study. Individuals with a history of neurological, visual, and motor problems (based on history and medical records) were excluded from the study.
Instruments and Procedure
This study was carried out in two phases. The first phase was dedicated to the development of the questionnaire. The development of the questionnaire involved three steps. The first step involved compilation of the item pool based on the feedback from adults who stutter and their significant someone (about various reactions faced by them), the opinions from the speech language pathologists, and the questionnaires presently available in the literature. The instruments that were refereed were those that have included a wide range of factors, including the speaker's fluency in different speaking situations, the speaker's confidence in different situations, the emotional and cognitive reactions that the speakers have to stuttering in different speaking situations, the speaker's opinions or attitudes about stuttering, and other factors.24,46,47 In the second step, the first draft of questionnaire was developed, which consisted of six domains targeting speech-related fear and anxiety, interpersonal and social relationships, behavioral reaction to stuttering, educational status, employment and job opportunity, and effect of speech therapy. Under each domain, there were sets of questions. Domain one (speech-related fear and anxiety) contained nine items pertaining to speech-related fear, avoidance, and anxiety in different speaking situations. Domain two (interpersonal and social relationships) contained four items that assess the difficulty faced by the speaker when communicating in a social situation, at home, and with friends. Domain three (behavioral reaction to stuttering) contained seven items with each item examining secondary behaviors of the speakers such as facial movement, clenching of fist, effortful breathing, etc. Domain four (educational status) contained five items that assess the problems faced by the speaker in class, with teachers, and in academics. Domain five (employment and job opportunity) contained eight items examining the degree of difficulty a speaker has when selecting a job and the difficulty faced by the speaker in the working environment. Domain six (effect of speech therapy) contained four items that assess the current status of stuttering, whether the fluency of speech has been improved or remained the same post therapy. For each item of the questionnaire, response scales were equipped so that greater scores indicated a higher degree of negative impact (2 for almost always) associated with stuttering and lesser scores indicated a lower negative impact (1 for sometimes and 0 for not at all). In the third step, the developed questionnaire was then subjected to content validity by obtaining ratings of seven speech language pathologists. The rating form for content validation required experts to provide their ratings in terms of relevance on a 5-point scale where a rating of 5 indicated an item to be extremely relevant and a rating of 0 signified the item to be not at all relevant. Based on the ratings obtained from the experts, the content validity index was calculated for further judgment about the items of the questionnaire. The second phase involved administering the validated questionnaire on the participants. All participants diagnosed with mild-to-moderate severity of stuttering were given a copy of the questionnaire and were instructed to fill the questionnaire themselves based on the response format provided (2—almost always, 1—sometime, and 0—not at all).
Analysis
Based on the scores obtained by the participants, the internal consistency and test-retest reliability of the questionnaire was estimated. For the estimation of the test-retest reliability, the questionnaire was readministered on 15% of the study population, ie, five subjects after one week of initial administration. Statistical analysis was carried out using a statistical package SPSS, Version 16.0. The details of goal-specific statistical analysis have been summarized in Table 1. The content validity index 48 was used to evaluate the content validity of the questionnaire as judged by the subject experts. The Cronbach's alpha was applied to estimate the internal consistency of the questionnaire, and paired t-test was used to estimate the test-retest reliability of the questionnaire. Further, descriptive statistics was used to understand the nature of reposes obtained from the study participants on the developed QOL questionnaire.
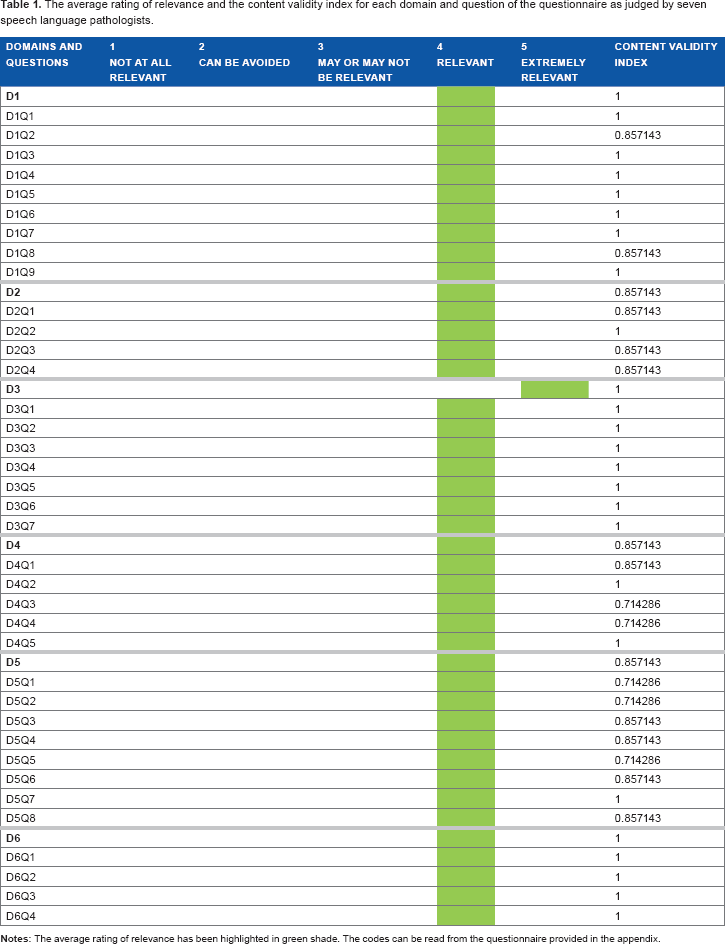
The average rating of relevance and the content validity index for each domain and question of the questionnaire as judged by seven speech language pathologists.
Results
The present study was conducted with an aim of developing a questionnaire to assess the QOL of people who stutter. The objectives of the study were to develop a questionnaire, perform a content validity of the same, and assess its test-retest reliability and internal consistency. The questionnaire consisted of 37 questions to be rated on a 3-point rating scale across six domains by people who stutter. The first draft of the questionnaire was given to seven speech language pathologists who rated the relevance of each domain and each question on a 5-point rating scale. The rating of 4 or 5 on the scale indicated a higher relevance of the entity, whereas the rating of 3, 2, or 1 indicated a lower relevance or no relevance. A content validity index was calculated for each domain and question, based on the average rating obtained by the seven speech language pathologists. The content validity index was calculated on the basis of the following formula:

The details of the average rating and content validity index of the questionnaire are provided in Table 1. The content validity index of greater than 0.8 was considered as being significant, which shows a high relevance of the entity for the target questionnaire.
As can be observed from Table 1, all the domains and questions had a content validity index of greater than 0.8 (indicating high content validity), except for D4Q3 (Do you feel stuttering is affecting your performance in academics?), D4Q4 (Does your stuttering have any influence on your relation with teachers and classmates?), D5Q1 (Do you think your stuttering has influenced your choice of occupation?), D5Q2 (Do you avoid participating in official meetings?), and D5Q5 (Do you think that you have limited career choices?).
The validated questionnaire was then given to 30 adults who stutter to rate their QOL across the six domains. The details provided in Table 2 depict the percentage distribution obtained for the rating of each question on the questionnaire.
The percentage distribution obtained for the rating of each question on the questionnaire by the adults with stuttering.
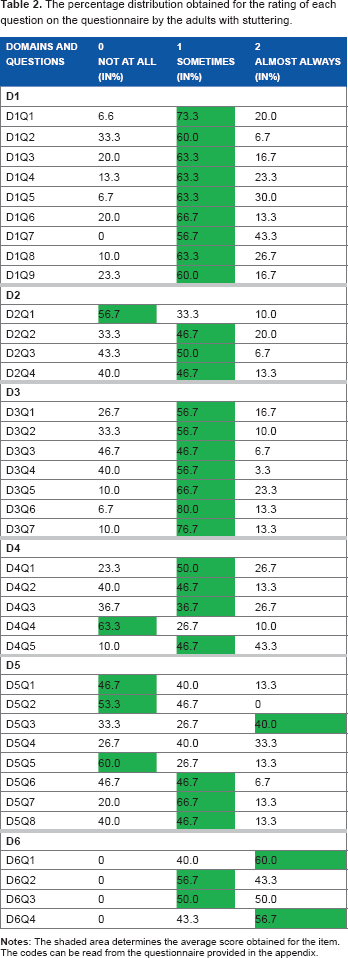
The results shown in Table 2 reveal that 29 (78%) out of 37 questions obtained an average score of 1, 3 (8%) out of 37 questions obtained an average score of 2, and 5 (13%) out of 37 questions obtained an average score of 0. When domain-specific analysis was performed, it was found that all the questions of domain one, ie, speech-related fear and anxiety, received an average score of 1. Therefore, it can be interpreted that all the participants of the study found speech-related fear and anxiety to be present sometimes. The analysis of domain two, ie, interpersonal and social relationships, revealed that except for D2Q1 (Do you avoid talking to opposite sex?), all other questions were present sometimes. The question coded D2Q1 was perceived as being not at all by the majority of the study participants. The scenario in the domain three, ie, behavioral reaction to stuttering, was similar to that obtained in domain one where all the answers indicated behavioral reactions to stuttering present sometimes. The analysis of domain four, ie, educational status, revealed that the problem of speaking in an academic setup was present sometimes except for question coded D4Q4. The item D4Q4 (Does your stuttering has any influence on your relation with teachers and classmates?) received an average score of 0 indicating not at all. The domain five, ie, employment and job opportunity, possessed scattered findings. Here, 50% of the questions obtained an average score of 1 indicating sometimes. The items coded D5Q1 (Do you think your stuttering has influenced your choice of occupation?), D5Q2 (Do you avoid participating in official meetings?), and D5Q5 (Do you think you have limited career choices?) were present not at all, experienced by 50% of the participants. The item coded D5Q3 (Did you choose a job where little speaking is required?) received an average score of 2, which indicates that the majority of the study participants selected a job on the basis of their speech competency. Among the questions of domain six, ie, effect of speech therapy, 50% of the participants indicated that the effect of therapy was present sometimes. The remaining two items, ie, D6Q1 (Are you currently attending or have you ever attended speech therapy for stuttering?) and D6Q4 (Do you feel your speech has improved after therapy?), received an average score of 2, ie, almost always, by the majority of the study participants, indicating their positive attitude toward speech therapy.
The scores obtained by the participants of the study were then subjected to the Cronbach's alpha for the estimation of the internal consistency. The details of the domain-specific internal consistency have been summarized in Table 3.
The overall and domain-specific internal consistencies of the questionnaire.

In the present study, internal consistency for all the domains tested was α > 0.50, indicating moderate internal consistency. Cronbach's alpha for the overall questionnaire including all six domains was α = 0.928, indicating that the overall internal reliability of the questionnaire was excellent.
For the estimation of the test-retest reliability of the questionnaire, the questionnaire was readministered on 5 out of 30 study participants. The paired t-test was administered on the scores obtained by the participants across the two trials to assess the presence of significant differences, if any. The details in Table 4 provide the domain-specific paired t-test results.
The domain specific t-value and P-value obtained from the comparisons of the scores of two trials by five participants.

The results of the paired t-test revealed that there was no significant difference between the scores obtained by the five participants across the two trials (P > 0.05). This indicates presence of good test-retest reliability for the various domains and questions of the developed questionnaire.
Discussion
Effect of stuttering on QOL of the affected individuals has recently gained the attention of researchers. Multidimensionality of the disorder is also reflected in multiple domains of life that get affected. There are a number of instruments available for determining the wide ranging aspects of stuttering, such as self-efficacy scale of stuttering, influence of stuttering on speaker's life, speech-related anxiety assessments,22,23,49 and OASES. 25 Each one of these tests has their own merits and demerits. All of these above-mentioned instruments would significantly enhance clinician's understanding about adults who stutter.
The present study was an attempt to explore the QOL of adults who stutter in the Indian regions. The design of the study was divided into two phases. The first involved the framing process of the questionnaire done with its content validity determined by the experts. The second phase involved the administration of the validated questionnaire on the participants of study to understand the profile of their QOL. Therefore, the discussion of results of the present research has been furnished in a similar sequence manner.
Framework of the Questionnaire, Content Validity, and Test-Retest Reliability
The questionnaire developed for the present study aimed at assessing the QOL of adults who stutter across multiple dimensions of life. Each dimension was categorized into a domain that involved a varying number of questions to determine the profile of the QOL. Specific factors that are addressed in the questionnaire are classified into domain one (speech-related fear and anxiety), domain two (interpersonal and social relationships), domain three (behavioral reaction to stuttering), domain four (educational status), domain five (employment and job opportunity), and domain six (effect of speech therapy). The questionnaire is designed in order to evaluate the totality of stuttering disorder based on the speaker perspective.
In the present study, the above-mentioned six domains were considered as they assess the spectrum of aspects of the stuttering disorder. Many adults who stutter report of existence of speech-related negative feeling, anxiety, and emotional tension. Clinically, there is consensus among therapists that anxiety is one of the many prompting, persevering, and precipitating factors that plays a part in stuttering. 50 Researchers and clinicians who work with adults who stutter reported that stuttering may have adverse effects on self-perception and, predominantly, on self-esteem. 51 Adults who stutter avoid many conditions in which they are likely to stutter. 52 The present research also addresses fear, anxiety, and avoidance behavior in different speaking situations. Educational settings give importance on presentations or verbal communication skills concentrating on community speaking and group interaction. 53 Students who stutter report of having problem in oral presentation, clarifying doubts in class, participating in discussions, etc. Therefore, inclusion of the domain on impact of stuttering on education was crucial. According to research, in many professions, fluent or effortless speech is one of the important aspects that helps enhance communication effectively, and so, often adults who stutter report that stuttering influences the selection of a career of their choice. 54 Hence, in the present study, employment and job opportunity is considered to be one of the domains that gives information about difficulties faced by people who stutter in a working environment.
The various domains and items that were generated in the questionnaire were subjected to content validity by seven experts from speech-language pathology discipline. The results depicted in Table 1 revealed that all questions had obtained relevant ratings by the seven experts. In addition to this, the content validation index was calculated for each domain and question by the described formula. As noted, two questions of domain four and three questions of domain five did not reach the critical content validity index. The questions that did not reach the critical content validity index were “Do you feel stuttering is affecting your performance in academics?”, “Does your stuttering have any influence in relation with teachers and classmates?”, “Do you think your stuttering has influenced your choice of occupation?”, “Do you think that you have limited career choices?”, and “Do you avoid participating in official meetings?” These five questions can be categorized into academics-related QOL and work-related QOL. There can be two reasons for low content validity index obtained for these questions. The first reason could be the apparent redundancy of these questions in relation to the other questions of the respective domains. But questions are different and hold their own significance for the QOL measurement. For example, the questions from the academic domain that have received low content validity index have been identified as being significant in literature. 36 Similarly, questions from the employment domain that have received low content validity index have been identified as being significant and decisive.36,38 The second reason could be the way some questions like “Do you feel stuttering is affecting your performance in academics?” were framed required more specificity. This also could have contributed to the low index. Thus, we believe that these questions, which have received a borderline content validity index, may overcome the threshold after certain rephrasing of questions is considered in future researches.
To estimate the test-retest reliability of the questionnaire, the questionnaire was readministered to 5 out of 30 study participants. The paired t-test was administered on the scores obtained by the participants across the two trials to assess the presence of significant differences. The results of the paired t-test revealed that there did not exist any significant difference between the scores obtained by the five participants across the two trials (P > 0.05). This indicates the presence of good test-retest reliability for the various domains and questions of the developed questionnaire.
The QOL Profile of Adults who Stutter
All the 30 participants of the study were given the developed questionnaire to assess their QOL associated with stuttering. The validated questionnaire consisted of 37 questions divided under six domains, which were to be rated on a 3-point scale. The score 0 was indicative of an event being not at all, the score of 1 signified an event being present sometimes, and the score of 2 indicated the event to be present almost always. As revealed by the results shown in Table 3, 29 (78%) out of 37 questions obtained an average score of 1, 3 (8%) out of 37 questions obtained an average score of 2, and 5 (13%) out of 37 questions obtained an average score of 0. Further, a domain-specific analysis was performed to understand the nature of this distribution.
Domain One (Speech-Related Fear and Anxiety)
This domain included questions pertaining to speech-related fear, avoidance, and anxiety in different speaking situations. The results depicted in Table 3 suggest that an average of 14% of the study population rated this domain as 0, 63% of the participants rated this domain as 1, and the remaining 21% preferred a rating of 2 for this domain. The average score for all the questions of this domain was also observed to be 1. This indicates that all the events referring to speech-related fear and anxiety were sometimes present. Also, it should be noted that a very small segment of the population is not experiencing speech-related fear and anxiety. This segment could be that part of the study group that either possessed mild stuttering or had a satisfactory psychological well-being to take care of the associated negative emotions. However, there is abundant literature support to justify the findings regarding the major segment of the population. Anxiety is considered a supplementary analytic feature of the stuttering disorder, particularly in adults. Anxiety in different social situations involves the persistent fear of humiliation and shame that restricts adults who stutter to participate in public conferences and social gathering. 55 Stuttering disorder is considered to have higher level of generalized anxiety, which results in severe distress and hinders day-to-day activities. Stuttering turns out to be more severe when exposed to challenging or threatening situations, for example, anxiety-provoking conditions such as speaking to a large group of listeners, speaking to a higher authority, or speaking to a listener who seems to be critical or uninterested. 2 Stuttering reduces when the situation is less threatening such as talking to family members and to a familiar person. A previous research suggests that adults who stutter had a significantly higher level of anxiety than controls when conversing on the telephone. 56 A study was done on 52 people with stuttering and 52 fluent speaking individuals by examining self-perceptions of depression, state anxiety, and communication attitude. 57 Findings of the study revealed that the anxiety level of adults who stutter is limited to their attitude toward communication situations and also response to negative communication experiences that they face in their daily life. The attitudes of 48 college-going students toward one of four constructs were studied, which included a factory worker who had fluent speech, a factory worker who stuttered, a lawyer who had fluent speech, and a lawyer who stuttered using an 81-item semantic differential scale. 58 The factory worker who stuttered reported of more insecurity, fear, and tension, and was observed to be more timid and weak than the factory worker who had fluent speech. Similarly, the factory worker who stuttered was judged to be less friendly, dominant, talkative, coordinated, and aggressive, and was observed to have poor self-confidence. The lawyer who stuttered was viewed more negatively than the factory worker who stuttered on 34 of the 81 items. The lawyer who stuttered was evaluated as more fearful, disordered, anxious, lazy, uncomfortable, dependent, and disorganized than the lawyer who did not stutter.
Domain Two (Interpersonal and Social Relationship)
This domain assesses the difficulty faced by the speaker when communicating in social situations, at home, and with friends. The results depicted in Table 3 suggest that an average of 43% of the study population rated this domain as 0, 44% of the participants rated this domain as 1, and the remaining 12% preferred a rating of 2 for this domain. Therefore, it can be noted that an equal proportion of the study group reported the impact of stuttering on interpersonal and social relationships to be either not at all or sometimes present. But the average score for all the questions of this domain was observed to be about 1. When question-specific analysis was done to identify the items that could have led to these findings, it was observed that the question “Do you avoid talking to opposite sex?” obtained a maximum score of 0. This indicates that 56% of the study population did not feel that their stuttering has prevented them from conversing to the people of the opposite gender. Again, these findings could be attributed to the gender-specific confidence levels of the individuals. Also, along with the gender of an individual, their age can be a confounding factor that the present questionnaire did not address. Therefore, further research on this could provide better insight and display the differences. Findings for the rest of the questions receive support from previous studies. A study was conducted on South African individuals in order to assess impact of stuttering on QOL of people who stutter. 36 Social life was considered an item to be assessed. A total of 16 subjects participated in the study, out of which 9 subjects reported that stuttering did not have much impact on their social well-being in terms of establishing friendships and 7 subjects reported that stuttering had either a positive or negative outcome on their social life.
Domain Three (Behavioral Reaction to Stuttering)
This domain included questions pertaining to behavioral reaction to stuttering. The results depicted in Table 3 suggest that an average of 24% of the study population rated this domain as 0, 62% of the subjects rated this domain as 1, and the remaining 12% preferred a rating of 2 for this domain. The average score for all the questions of this domain was observed to be 1. This indicates that all the events referring to behavioral reaction to stuttering were sometimes present. It is also noted that very few participants of the study did not experience the behavioral reaction to stuttering. In all, 80% of the participants reported to have effortful repetition of syllables, sounds, words, or phrases. A self-report test method and behavior checklist was administered to 42 people who stutter and 76 people who did not stutter in order to examine the occurrence and nature of the reactions that they apparently used to cope with the anticipation. 59 Adults who stuttered reported greater amount of speech-related coping responses than non-stutterers. A factor analysis showed a significant difference in nature and type of coping responses in adults who stutter when compared to non-stuttering participants. This finding proposes that coping responses of adults who stutter and non-stutters are hypothetically useful with respect to differential diagnosis and management. Adults who stutter will use starter devices that help them get a running start in preparation for the feared word. Timing devices such as eye blinking, stamping a foot, or tapping a finger often fall into this category. Finally, adults who stutter sometimes try to disguise or cover up their stuttering so that it is less noticeable to listeners. Behaviors such as turning one's head away while talking, putting a hand over the mouth while talking, laughing, and talking at a very fast rate or at a very low volume may fall into this category.
Domain Four (Educational Status)
This domain assesses difficulties faced by the students in class, with teachers, and in academics. The results depicted in Table 3 suggest that an average of 34% of the study population rated this domain as 0, 41% of the subjects rated this domain as 1, and the remaining 24% preferred a rating of 2 for this domain. The question-specific analysis revealed that all the questions except for the question “Does your stuttering have any influence on your relation with teachers and classmates?” were found to be present sometimes. The question on relation with teachers and classmates received an average score of 0, ie, not at all. This probably could be because of two reasons. First, the participant has learnt to avoid the situations, thus not encountering the effect. Otherwise, the most probable reason could be the understanding environment that one must be facing. There are evidences that suggest that young adults put greater trust on their friends than their parents with respect to the reactions linked with stuttering. 60 The effect of stuttering on educational status has been described by many researchers in the past. Studies report that students with stuttering were more disliked and excluded than their non-stuttering peers in the group activities and were also ignored in the social activities, and not allowed to take part with their peers. 61 A study was conducted on 16 participants, out of whom 6 reported that their stuttering had no effect on their educational performance and relationship with their teachers, while 10 reported that stuttering had a negative impact on their educational performance and relationship with their teachers to a greater or lesser extent. 36 In all, 10 students who reported of having problems with academic performance had difficulty in oral presentations, reading aloud, and poor self-confidence. Students who stuttered had difficulty in maintaining friendship with peers; the main reason for this was teasing, which had a negative impact on students who stutter. Another study revealed that 80% of the students who stutter face peer aggression and about 95% of the students face aggression from their teachers because of their stuttering. 62
Domain Five (Employment and Job Opportunity)
This domain examines the degree of difficulty a speaker had when selecting a job and also assesses the difficulty faced by the speaker in a working environment. The results depicted in Table 3 suggest that an average of 40% of the study population rated this domain as 0, 42% of the participants rated this domain as 1, and the remaining 16% preferred a rating of 2 for this domain. Here, 50% of the questions obtained an average score of 1. The questions “Do you think your stuttering has influenced your choice of occupation?”, “Do you avoid participating in official meetings?”, and “Do you think you have limited career choices?” received a majority score of 0. The question “Did you choose a job where little speaking is required?” received an average score of 2, which indicates that the majority of the study participants selected a job on the basis of their speech competency. Therefore, the reasons behind the three questions that received a score of 0 become clearer. As majority of the participants in the present group selected the jobs as per their speech competency, their speech fluency never would have got taxed to encounter a breakdown in a work situation that would force them to avoid meetings. A study reported that stuttering had an influence on occupation. 36 Adults who stutter report of having difficulty at the workplace in maintaining relationships with supervisors or managers and coworkers, and there was very less chance for promotion. In a survey with 282 adults who stutter, 16% of them were not employed in a job because of their stuttering; more than half of adults who stutter stated that their talents were not being noticed because of stuttering. 63 Previous research reveals that adults who stutter were not permitted to apply for promotions because of stuttering. 5 There are also studies that report that 50% of respondents had not been asked to accomplish certain speaking tasks that were typically required of someone in their position. 64
Domain Six (Effect of Speech Therapy)
This domain assesses the current status of stuttering, whether the fluency of speech has been improved or remained the same post therapy. The results depicted in Table 3 suggest that none of the study participants rated this domain as 0, 47% of the participants rated this domain as 1, and the remaining 52% of the participants preferred a rating of 2 for this domain. Among the questions of domain six, 50% of the questions received an average score of 1. The remaining two items, ie, “Are you currently attending or have you ever attended speech therapy for stuttering?” and “Do you feel your speech has improved after therapy?” received an average score of 2, ie, almost always, by the majority of the study participants, indicating their positive attitude toward speech therapy. This could be attributed to the fact that all the participants who were recruited for the present study were either undergoing or had undergone the speech therapy sessions that had led to a good progress in their fluency status. A study was conducted to assess the effectiveness of stuttering therapy for adults. 65 A total of 16 subjects participated in this study. Evaluation was done nine months prior to the therapy, again when therapy was initiated, at the end of nine-month therapy period, and then nine months after the completion of therapy. There was a statistically significant result. When severity was taken into consideration, the more severe group showed significant improvement during therapy, but slight relapse was seen during the follow-up period. The less severe group improved during therapy, and improvement was also seen during the follow-up period. A study reported that out of 15 participants who underwent therapy, 14 participants reported that speech therapy was not helpful and only 1 participant reported the speech therapy as being beneficial in terms of enhancing fluency. 36
Overall, the findings of the present study suggest that there were 5 out of 37 questions that received lower content validity index and there were 5 out of 37 questions that were found to be impacting the people who stutter. We performed an analysis of these two observations and realized that 4 out of 37 questions had both low content validity and low impact score. These items were D4Q4 (Does your stuttering have any influence on your relation with teachers and classmates?), D5Q1 (Do you think your stuttering has influenced your choice of occupation?), D5Q2 (Do you avoid participating in official meetings?), and D5Q5 (Do you think that you have limited career choices?). Therefore, the usage of these questions in future appears confusing. Either these questions require rephrasing or they were not having any effect because of the coping and avoiding behaviors observed among individuals with stuttering. However, based on the trends observed in the existing questionnaires and the strong literature support for the link between these questions and stuttering, we recommend their inclusion for future usage. The rest of the framework of the questionnaire has been successful in providing the QOL profile of the people who stutter in the present study. Thus, it may be promising to use it in future research to further understand the complicated nature of stuttering and its impact.
QOL of Adults who Stutter and the Sociocultural Factors
The emotional reactions, such as fear, anxiety, frustration, shame, and embarrassment, that are associated with stuttering have been reported to be universal in nature. They do not seem to vary much across cultures. 29 Therefore, the findings obtained from the subjects of the present study with respect to speech-related fear and anxiety as assessed from domain one of the questionnaire hold valid. A study explaining sociocultural issues with respect to stuttering stated that adults who stutter are viewed as if they have a disease instead of having a communication disorder. 29 This study also states that some Asian Indians believe that it is appropriate to hide a disability from public view since his/her disability is seen as a reflection of the entire family. In other cultures such as Greek, Arab, and Chinese, Adults who stutter (AWS) are treated as if they are abnormal or less of a person. They are not offered the same opportunities as others and are affected by discrimination in many areas of life.29,36 There are domains in the questionnaire of the present study that reflects these issues: the domain on interpersonal and social relationships, the domain on educational status, and the domain on employment opportunities. Contrary to the statement raised by the previous study on Asian Indians, the present study on Asian Indians did not reveal any significant limitation by AWS with respect to educational and employment statuses. There seem to be concerns in AWS about limited career opportunities, and at the same time, the impact of stuttering at work or educational location is seen only sometimes. These differences in the reported study and the present study could be attributed to two reasons: first, the changes in Indian culture and perspectives in opening better opportunities for the individual with communication disability, and second, the multicultural diversity of India cannot be generalized—it varies geographically. However, the majority to the trends revealed in the present study possess a similarity with QOL data of AWS from other cultural regions.
Overall, the present study has been able to project certain trends of QOL among AWS in an Indian region. However, the present study has its own limitations. First, the QOL data obtained in the study is specific to a South Indian district and cannot be considered as a representation of QOL of AWS from the entire nation. Second, the cultural differences in India are vast, and deriving a national conclusion in this paper might not be appropriate at this stage. It is true that the there is a cultural shift being observed in India, but it is yet to spread nationally. Lastly, the questionnaire used in the present paper, to assess the QOL, might need further modifications based on the data obtained before it gets standardized for clinical utilization.
Conclusion
The aim of the present study was to explore the QOL of adults who stutter in an Indian region. The questionnaire developed in the present study for this purpose enabled exploring the multi-dimensionality of stuttering and its impact on the participants. Though there was variability across the multiple domains, a common observation across the data was that stuttering did not spare even one domain of life. With respect to the cultural aspects specific to India, the QOL data were not very distant from the QOL data obtained regarding adults who stutter in other cultural settings. The results also suggested an emerging trend of better acceptance by the society of AWS, marking a significant shift in the cultural aspects among the people there. Even though the AWS continue to anticipate a sense of discrimination and insecurity with respect to their social participation, their actual QOL in a social situation is not severely affected. There can be crucial issues while counseling the AWS to change their negative perspectives toward social reactions. However, we also emphasize the fact that these observations are made from 30 AWS in one South Indian district of India. India being a multicultural country possesses intensive cultural differences within the distance of a few miles. Therefore, these findings should not be generalized directly. A further research with respect to different Indian cultural and socioeconomic settings may provide a promising database.
Author Contributions
ALV and GB were involved in the idea formulation and manuscript preparation. JD contributed in the data collection and preparation of the questionnaire. JSB made critical revisions and approved final version. All authors reviewed and approved of the final manuscript.