
Abstract
Background
The aim of this study was to investigate the rehabilitative process and visual rehabilitation outcomes in patients with central vision loss due to age-related macular degeneration (AMD).
Methods
Ninety-five subjects with AMD selected from the attendees of the National Centre of Services and Research for the Prevention of Blindness and Rehabilitation of Low Vision Patients—International Agency for Prevention of Blindness—IAPB Italia Onlus, were evaluated for this retrospective study. Low vision examination included psychological counseling, best corrected visual acuity (BCVA), near visual acuity, Pelli-Robson contrast sensitivity, and fixation stability analysis. Once the clinical assessment was completed, patients attended a low-vision rehabilitative pathway based on visual stimulation, devices training and, if needed, psychological support. Required magnification and reading speed were also evaluated.
Results
For the whole sample, the mean BCVA of the better eye was 0.7 (±0.2) LogMAR and of the worse eye was 1 (±0.2) LogMAR. Restoring reading ability was the most important focus for the patients examined as it was requested by 85% of the whole sample. Mean power of optical magnifying aids for near activities was 10.6 (±9.1) positive spherical diopters. Mean reading speed for the whole sample was 33.1 (±18.2) words per minute (wpm) before visual rehabilitation sessions and increased to 55.2 (±33.1) wpm after visual rehabilitation path. To cope with distance difficulties, 78 distance refractive correction, 10 Galilean telescopes, and 7 Keplerian telescopes were prescribed. For intermediate distance activities, 22 compensation lenses and 10 Galilean telescopes were suggested. Moreover, PC magnifier softwares were prescribed to nine patients. Sixty-five polarized medical filters were prescribed to reduce glare of sunlight. Because of unstable fixation in their better eye (32.3% (±19.7) within 2° circle and 54.8% (±22.9) within 4° circle) and visual acuity < 1.2 LogMAR in the fellow eye, 38 subjects, before starting the devices training sessions, attended a bio-feedback rehabilitation session with flickering pattern stimulus. In these subjects, fixation stability increased significantly to 75.6 (±14.9) within 2° and 89.4 (±19.5) within 4° (P < 0.05), respectively.
Conclusions
Attending a customized low-vision intervention based on a multidisciplinary approach seems to be effective for improving visual functions in AMD. Both optical/electronic magnifiers and specific visual stimulation program can enhance visual performances.
Keywords
Introduction
Age-related macular degeneration (AMD) is the most common leading cause of low vision among the elderly in developed countries.1–5 The prevalence of AMD in the United States is expected to increase to 3.0 million in 2020.6,7 AMD involves the central part of the retina resulting in a progressive central vision loss. During the course of the disease, people with AMD develop an absolute central scotoma (area with absent or poor vision) with loss of foveal stable fixation. In order to view, subjects develop a new fixation point, called preferred retinal locus (PRL) in an eccentric part of the retina that can be accurately defined by means of microperimetry (fundus-related perimetry).8–11 The advanced stage of AMD leads to distortion of vision, reduction of both visual acuity and contrast sensitivity (CS), and glare. Given this, people with visual impairment because of AMD are unable to perform activities of daily living (ADLs), such as recognizing faces, reading, and watching television, resulting in a poor patient's quality of life. It is well documented that changes in lifestyle because of AMD can determine many difficulties and create feelings of inadequacy and emotional distress resulting in a psychological burden. 12 In addition, a study by Hayman et al reported that visually impaired older adults have higher level of depressive symptoms than adults without low vision. 13 Although medical therapies have been developed and improved in order to contrast the loss of central vision,14–20 vision rehabilitation is the only treatment option to date for restoring patients' independence during ADLs and to improve their quality of life.21,22 In particular, in order to compensate visual acuity reduction due to central scotoma, visual rehabilitation intervention usually involves different types of magnifying devices. 23 The aim of this retrospective study was to evaluate visual rehabilitative procedures—in a multidisciplinary centre—and the outcomes of visual rehabilitation in patients affected by AMD. Moreover, we assessed the low-vision aids provided in order to cope with patients' difficulties in daily life activities.
Methods
Subjects
A retrospective review was carried out in 95 patients with AMD (38 females, 57 males; mean age: 79.7 years, range: 65-92 years) from the attendees of the National Centre of Services and Research for the Prevention of Blindness and Rehabilitation of Low Vision Patients, IAPB Italia Onlus, in Rome. Patients were referred to our centre to attend a low-vision rehabilitation intervention in order to cope with visual disabilities during their daily life. Subjects with AMD rehabilitated from January 2011 to January 2012 were selected on the basis of the following clinical criteria: a best corrected visual acuity (BCVA) between 1 logMAR and 0.5 logMAR and bilateral central vision impairment. Exclusion criteria included any other concomitant eye disease, cognitive impairment defined by means of mini-mental state examination administered by the psychologist during the first assessment, significant media opacities, and ocular surgery in the previous six months. Subjects who had access to our low-vision rehabilitation center were informed by our staff about the likelihood of using their own clinical data for research purposes. Every patient gave their own informed consent. Because of the retrospective nature of this research, ethical approval was not required. The research was approved by the scientific board of the IAPB Italia Onus.
National Centre of Services and Research for the Prevention of Blindness and Rehabilitation of Low Vision Patients: Rehabilitation Protocol
The National Centre of Services and Research for the Prevention of Blindness and Rehabilitation of Low Vision Patients rehabilitation (International Agency for Prevention of Blindness-IAPB, Italia Onlus) has a multidisciplinary team comprising psychologists, ophthalmologists, orthoptists, an orientation and mobility teacher, and an expert in typhlology. As a standard procedure, low-vision assessment included psychological counseling, complete ophthalmological examination, microperimetric evaluation, low-vision devices training, and lastly, prescription of low-vision aids. First, in order to better define patients' needs, the psychologist provided a specialized assessment. The psychologist supported patients in focusing on personal goals in order to facilitate independence in ADLs. BCVA was measured by ophthalmologist by means of the Early Treatment Diabetic Retinopathy Study (ETDRS) charts (Precision Vision, Bloomington, IL) and recorded as logMAR at a distance of 4 m with the best optical correction in a normal room illumination. Near visual acuity was determined monocularly using the Italian version of the MNRead Acuity Charts adding +4 spherical diopters. CS was measured using the Pelli-Robson CS charts adding to the best correction for distance +1 spherical diopter. Fixation analysis of the PRL was performed by means of MP1 Microperimeter (Nidek Technologies, Padua, Italy). As a result, both PRL location and stability were classified according to Fujii classification. 24 During the multidisciplinary briefing, as a matter of routine, the team discussed the intervention approaches to help patients deal with the difficulties of daily living. On the basis of both patients' residual visual function and needs, a customized rehabilitation program was identified for each patient. Therefore, the visual rehabilitation procedure, the likelihood of a psychological counseling during low-vision intervention, the most appropriate devices to train the patients with, and the number of rehabilitation sessions were established. Patients with unstable and relatively unstable fixation (Group A) were initially treated with biofeedback visual stimulation at the MP1 Microperimeter in order to improve fixation stability before starting devices training with a certified orthoptist. Biofeedback stimulation with a pattern stimulus was performed according to the procedure described elsewhere. 25 On the other hand, patients with a stable fixation (Group B) were able to start the devices training sessions. Devices training session was performed by a certified orthoptist in order to teach patients how to correctly use and handle magnifying devices and to suggest strategies to perform daily living tasks independently. In particular, to restore reading ability, visual rehabilitation training sessions focused on identifying the most suitable device for reading, managing the device, and teaching page navigation strategies. Patients attended training sessions of 1 hour once a week. On average, three sessions were required. Moreover, if needed, training sessions could be associated with psychological support in order to provide special support for patients who also have depression due to eye disease, encourage patients, and enhance the effectiveness of rehabilitation. Reading speed was calculated by counting the number of correct words read in 1 minute (words per minute [wpm]) on an Italian newspaper article with the appropriate low-vision device. According to patients' needs, appropriate low-vision devices were prescribed once the low-vision rehabilitation program was completed.

The diagnostic and rehabilitative path of the National Centre of Services and Research for the Prevention of Blindness and Rehabilitation of Low Vision Patients.
Outcomes and Parameters Measured
For this retrospective review, data were extracted from low-vision clinical charts and included patients' needs, BCVA, near visual acuity (NA), Pelli-Robson CS, fixation stability, type of assistive magnifying device prescribed, and reading rate magnified-assisted evaluation. The previous data were administered by the certified orthoptist.
Statistical Analysis
Patients' data were collected and stored in an Excel (Microsoft) sheet database. A descriptive analysis of the sample was performed, including means and SD. Patients were divided into two groups according to the visual rehabilitation program undertaken. To assess whether the difference between pre and post visual rehabilitation outcomes (fixation stability and reading performance (for Group A) was significant, the analysis of variance for repeated measures was carried out for Group A. In order to examine the significance of the reading speed before and after the rehabilitative pathway in Group B, a paired t test was used. Moreover, in order to verify the relationship between fixation stability and reading speed for Group A, a linear regression analysis was performed. Statistical significance was set at P ≤ 0.05.
Results
A review was conducted for all the patients who met the inclusion criteria defined above. A total of 95 subjects were analyzed; 38 (40%) females and 57 (60%) males were included with a mean age of 79.7 (±7.7) years. The mean BCVA of the best eye was 0.7 (±0.2) logMAR while that of the worse eye was 1 (±0.2) logMAR. A total of 16 subjects had an equal BCVA in both the eyes. In summary, Table 1 shows the clinical parameters collected for the whole sample.
Clinical parameters of patients evaluated for this retrospective.

Table 2 shows patients' needs expressed during the first psychological evaluation. Resuming and optimizing reading ability was the most important goal for patients examined and it was requested by 85% of the whole sample.
The most important demands for 95 patients with AMD.

Figure 2 represents the distribution of low-vision devices prescribed for near activities.

Distribution (number: y axis) of low-vision devices for near activities in 95 subjects with AMD.
Magnification power of optical magnifying devices for near activities had a mean of 10.6 (±9.1) positive spherical diopters. Mean reading speed for the whole sample was 33.1 (±18.2) wpm and it increased to 55.2 (±33.1) wpm after visual rehabilitation program.
For coping with distance difficulties, 78 distance refractive correction, 10 Galilean telescopes, and 7 Keplerian telescopes were prescribed. On the other hand, to resume visual tasks for intermediate distance, 22 compensation spectacle and 10 Galilean telescopes were suggested to use. In order to use personal PC without any difficulties, nine patients were prescribed PC magnifier software. Sixty-five polarized medical filters were prescribed to reduce glare of sunlight. Only one patient reported no advantage of polarized filters. Moreover, with reference to Pelli-Robson test, a proper lamp was suggested to those patients who had a poor CS.
More interestingly, 38 subjects (Group A) of the whole sample attended 10 stimulation sessions of biofeedback with flickering pattern stimulus, before devices training sessions. Because of a wide lesion in the fellow eye and a best corrected visual acuity less than 1.2 LogMAR, these subjects were trained monocularly. Patients of Group A showed an unstable fixation: 32.3% (±19.7) within 2° circle and 54.8% (±22.9) within 4° circle; therefore, a biofeedback stimulation with flickering pattern stimulus was suggested. Fixation stability improved to 75.6 (±14.9) within 2° and to 89.4 (±19.5) within 4° (P < 0.05, respectively). Once the stimulation sessions were completed, patients started the devices training sessions, for improving the needs required. For near tasks, the following were prescribed for Group A: 20 monocular magnifying glasses, 7 aplanatic lenses, 6 closed-circuit televisions (CCTVs), and 5 hand-held magnifiers. A significant improvement was also found in reading ability: patients read newspaper with a mean reading speed of 27.6 (±9.8) wpm and 51.4 (±23) wpm (P < 0.05). On the other hand, the other 57 subjects (Group B) were rehabilitated in both the eyes. For near tasks, 43 patients of Group B were rehabilitated and 22 high plus reading lenses, 15 CCTVs, and 6 prismatic magnifying spectacles were prescribed. Mean reading speed was 31.7 (±12.6) wpm before visual rehabilitation and it increased to 51.9 (±27.6) wpm (P < 0.05) after rehabilitative pathway (Figs. 3A,B).
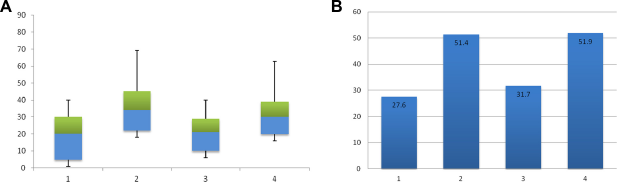
Box plots (
As Figures 4A and B show, a positive correlation was found between both improvement of fixation points falling within 2° and 4° diameter circles on the mean fixation position and improvement in reading speed (r = 0.31 and r = 0.25, P < 0.05 respectively). Improvement in fixation stability and reading speed were determined by subtracting the data collected at the end of the rehabilitative intervention with those recorded before the start of rehabilitation.

Linear regression: change of reading speed as a function of change in fixation stability as the percentage of fixation points falling within 2° (
Discussion
AMD is one of the major causes of visual impairment, leading to central vision loss and inability to perform many ADLs. The main goal of visual rehabilitation process is to allow visually impaired people to cope with visual disability and to reprise performing daily living tasks independently. In patients with AMD, restoration of near activities, such as reading, is the most important focus for working, leisure purposes and to being involved in everyday life. Therefore, reading is a great challenge for both visually impaired subjects and low-vision rehabilitators. The aim of this study was to evaluate the visual rehabilitation process and the outcomes of rehabilitative pathway in patients with the most common cause of severe visual impairment in industrialized countries. The most important aspect of this study is that our Low Vision Rehabilitation model is based on the work of a multidisciplinary team for addressing various tasks identified by the patients. Although many publications on this topic described training protocols and effectiveness of low-vision devices,21,22,26 we would to highlight the importance of a customized and multidisciplinary rehabilitative approach for assisting visually impaired people. In particular, the psychologist helps patients to deals with problems related to visual disability and supports them for achieving emotional well being. As reported by several authors, vision impairment can affect psychological status resulting in the onset of depressive symptoms that can lead to a ruinous rehabilitation pathway.12,27 Therefore, psychological support seems to be fundamental for allowing patients to achieve their goals. However, in our study, we can assume the importance of psychologist only on patients' own satisfaction and not basing on standardized quality of life questionnaire. Unfortunately, this paper does not provide a review of quality of life questionnaire as an indicator of patient satisfaction and multidisciplinary visual rehabilitation effect. Remarkably, resuming and optimizing reading ability were the main focuses for 85% of our patients. According to other studies, people with central vision loss can achieve good reading speed by attending a visual rehabilitation program based on both eccentric view training (biofeedback stimulation) and magnification through low-vision devices. 25 As suggested by several research groups, fixation stability is related to reading performance; therefore, patients with an unstable fixation read more slowly than those with stable fixation.27,28 For this reason, in order to improve fixation, patients with poor ability to fixate (Group A) were trained with biofeedback stimulation. The results we obtained indicate that visual stimulation by means of microperimeter MP1 can significantly increase fixation stability in patients with central scotoma and a poor ability to fixate a target due to AMD. Therefore, we could suggest that patients with AMD and poor fixation stability should attend a rehabilitation program based both on eccentric view training and biofeedback stimulation, in addition to device training. The results of our study confirm that biofeedback stimulation allows patients to better manage the PRL. Visual stimulation plays an important role in the mechanisms of cortical reorganization and vision restoration, representing an implementation of new training methods. In the future, it would be recommended to researchers to increase clinical trials in this interesting field, also for applying visual stimulation procedures in patients with other diseases as well. Moreover, as reported in the literature, magnifying aids represent the only solution of allowing patients to read without any difficulty. 29 Since, there is no standard procedure for visual rehabilitation of patients with AMD, an important aspect of this study was the highlight given to the combination of stimulation session with devices training as rehabilitative pathway. Therefore, we would emphasize that attending a visual rehabilitation program composed by visual stimulation, corresponding to a specific training for using residual vision, and low-vision aids could represent an appropriate useful visual rehabilitation program. In order to compensate for visual acuity reduction, providing magnifying devices in these patients is confirmed to be the most appropriate form of intervention for near, intermediate, and distance activities.30,31 In the literature, the beneficial effect of optic or electronic devices for reading ability and near tasks is well known, but to date not so much data have been published to identify the appropriate aids for recovering patients' independence for distance visual activities. Another intent of this study was to clarify that the first step of visual rehabilitation process, in order to enhance distance visual acuity, is not identifying magnifying telescope but correcting refractive errors. This seems to be in accordance with Markowitz's assertion that there is a high prevalence of uncorrected refractive errors among patients with low vision and the best refractive correction seems to be one of the best rehabilitative solution for far distance activities. 32 Another important aspect worth highlighting is the high percentage of polarized medical filters prescribed; the main function of medical filters is to protect the visual system from harmful radiations and to contribute to the improvement of visual comfort.33,34 As many studies reported, they seem to represent a valid low-vision device for reducing glare caused by artificial and natural light sources and for increasing contrast vision as well.35–37 This combination of findings seems to have important implication for developing customized vision rehabilitation pathway.
Finally, a number of important limitations need to be considered. First, we do not analyze any further data on the long-term effect of visual rehabilitation. Therefore, the study is limited by the lack of information about follow up. In conclusion, we can assume that in patients with AMD, a good visual rehabilitation program should be performed by a multidisciplinary team. Moreover, patients' needs can be achieved by providing appropriate optical or electronic magnifiers and by attending a special visual stimulation program to enhance visual performance.
Author Contributions
Conceived and designed the experiments: FMA, SF, VS, MS, AP, ST. Analyzed the data: FMA, SF, VS, MS, AP, ST. Wrote the first draft of the manuscript: FMA, SF, VS, MS, AP, ST. Contributed to the writing of the manuscript: FMA, SF, VS, MS, AP, ST. Agree with manuscript results and conclusions: FMA, SF, VS, MS, AP, ST. Jointly developed the structure and arguments for the paper: FMA, SF, VS, MS, AP, ST. Made critical revisions and approved final version: FMA, SF, VS, MS, AP, ST. All authors reviewed and approved of the final manuscript.